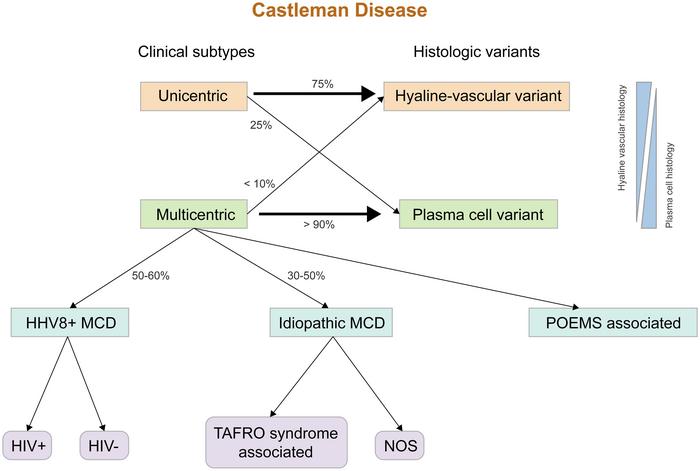

Castleman disease (CD) is an intriguing and rare lymphoproliferative disorder characterized by an array of histological and clinical manifestations. As a non-clonal hematological disorder, Castleman disease presents diagnostic challenges due to its intricate pathology and its potential overlap with other lymphoproliferative conditions. This complexity is reflected in its classification, which divides CD into unicentric (UCD) and multicentric (MCD) forms, each with unique clinical implications.
Unicentric Castleman disease typically presents with localized lymphadenopathy, often asymptomatic, which contributes to its subtlety in diagnosis. Unlike multicentric forms, UCD is primarily characterized by solitary lymph node enlargement, allowing patients to escape early detection unless the enlargement becomes significant. Conversely, multicentric Castleman disease is marked by more severe systemic symptoms, including fever, night sweats, and weight loss, creating a complex clinical picture that often leads to delayed diagnoses.
The distinction between the two forms of CD hinges on their histopathological characteristics. Histologically, unicentric disease is generally associated with hyaline vascular (HV-CD) or plasma cell variants (PC-CD). HV-CD is defined by regressed germinal centers and a distinctive “onion-skin” appearance due to concentric mantle zones surrounding sclerotic blood vessels. Meanwhile, plasma cell variants exhibit sheets of plasma cells interspersed with vascular proliferation, making identification crucial in dictating treatment options.
The variability in pathology extends to molecular findings and cytogenetics. Interestingly, evidence suggests clonal cytogenetic abnormalities within HV-CD, hinting at a potentially neoplastic origin associated with follicular dendritic cells. These genetic anomalies underscore the necessity for thorough molecular characterization when diagnosing and managing these patients. In unicentric cases, commonly detected mutations include PDGFRB N666S, while idiopathic multicentric Castleman disease is associated with mutations in genes such as NCOA4, SETD1A, and DNMT3A. These genetic insights further emphasize the multifaceted nature of CD and its underlying pathophysiology.
Diagnosis of Castleman disease necessitates a careful interplay of clinical presentation, imaging, laboratory investigations, and definitive histopathological findings. The histological diagnosis is paramount in distinguishing HV-CD from PC-CD. The presence of vascularized regressed follicles with fibrotic stroma is indicative of HV-CD, while the diagnosis of PC-CD mandates the identification of interfollicular plasmacytosis and a careful exclusion of other conditions through rigorous laboratory evaluation.
The mimicry exhibited by various conditions poses considerable challenges to the diagnosis of CD. Lymphomas, particularly follicular hyperplasia and angioimmunoblastic T-cell lymphoma, may closely resemble the histologic landscape of HV-CD, complicating the determination of an accurate diagnosis. Classic Hodgkin lymphoma, particularly in its interfollicular variant, presents additional hurdles, as the overlap with PC-CD can obscure the identification of Reed-Sternberg cells—central to the diagnosis of Hodgkin lymphoma.
Moreover, plasma cell neoplasms exhibit features echoed in PC-CD, particularly when a monotypic plasma cell population is present. The differentiation from IgG4-related disease is particularly pertinent, as it often presents with similar histopathological characteristics but necessitates distinct therapeutic approaches. Autoimmune conditions like rheumatoid arthritis and lupus also present a clinical overlap, resulting in Castleman-like lymphadenopathy that requires careful diagnostic stratification.
Importantly, the clinical implications of CD extend beyond its immediate presentation, with associated neoplasms representing a significant concern for affected patients. Research has demonstrated an increased risk of hematologic malignancies, including various lymphomas, in individuals with Castleman disease, particularly those presenting with multicentric variants associated with HHV8 and HIV infection. This interplay between Castleman disease and malignancy underscores the necessity for continued vigilance and monitoring in affected individuals.
The neoplastic potential of Castleman disease is further illustrated by associations with conditions such as Kaposi sarcoma, particularly in patients with multicentric forms of CD. The overlapping pathophysiological mechanisms linked to immune dysregulation and viral oncogenicity, specifically in HHV8-positive patients, complicate the clinical management of these patients.
Given this complex clinical landscape, multicentric Castleman disease often demands a multidisciplinary approach integrating the expertise of pathologists, oncologists, and infectious disease specialists. Careful consideration of clinical features alongside histopathological analysis and molecular investigations can facilitate an accurate diagnosis, thus allowing for timely and targeted therapeutic interventions.
Definition and precise understanding of Castleman disease remain essential in advancing research aimed at unraveling its pathogenesis and improving patient outcomes. Ongoing studies focused on the molecular underpinnings and therapeutic strategies are critical for refining the clinical management of this enigmatic disorder. There is a growing consensus that understanding the interactions between Castleman disease and its mimickers is essential for enhancing diagnostic accuracy and management for those affected.
In conclusion, Castleman disease embodies the spectrum of complexity found in lymphoproliferative disorders. Its diverse presentations, overlapping similarities with mimicking conditions, and associations with various neoplasms necessitate a comprehensive approach to diagnosis and management. The dynamic interplay between clinical features and molecular pathology underscores the importance of continued research efforts to elucidate the underlying mechanisms of Castleman disease, paving the way for improved therapeutic strategies and outcomes.
Subject of Research: Castleman Disease and Associated Neoplasms
Article Title: Mimickers and Associated Neoplasms of Castleman Disease
News Publication Date: 24-Mar-2025
Web References: https://www.xiahepublishing.com/2771-165X/JCTP-2024-0004
References: 10.14218/JCTP.2024.00047
Image Credits: Credit: Xiaohui Zhang
Keywords: Castleman disease, lymphoproliferative disorder, histopathology, neoplastic origin, diagnostic challenges, multicentric, unicentric, lymphoma, plasma cells, HHV8, autoimmune conditions.
Tags: Castleman diseasediagnosis challenges in Castleman diseasehistopathological characteristicshyaline vascular variantlymphadenopathy in Castleman diseaselymphoproliferative disordersmulticentric Castleman diseaseplasma cell variantrare hematological disorderssystemic symptoms of Castleman diseasetreatment options for Castleman diseaseunicentric Castleman disease


{kind=link}