ELCC 2019 (European Lung Cancer Congress), April 10-13, Geneva, Switzerland
Credit: © European Society for Medical Oncology
Geneva, Switzerland, 10 April 2019 – Two studies to be reported at ELCC 2019 (1,2) provide new insights on the efficacy and safety of immunotherapy in elderly patients with advanced non-small-cell lung cancer (NSCLC), where information has previously been lacking despite being the age group most commonly affected.
Immunotherapy with drugs that target immune pathways to enhance the body’s ability to recognise and destroy tumour cells is emerging as an effective treatment option for patients with advanced NSCLC (3). Although around half of all people newly diagnosed with NSCLC are elderly (4) there is currently limited evidence on the efficacy and safety of immunotherapy in this age group because they have been under-represented in clinical trials. There have also been concerns that age-related decline in the immune system might affect the efficacy of immunotherapy in older patients.
Real-life study suggests shorter overall survival with immunotherapy in elderly
A retrospective study of patients with advanced NSCLC treated with immunotherapy in real-life clinical practice (1) suggested that elderly patients (greater than equal to 70 years) may have shorter overall survival than younger patients but demonstrated that toxicity was similar.
Researchers retrospectively reviewed all patients with advanced NSCLC treated with immunotherapy agents at Hospital Universitario Ramon y Cajal in Madrid, Spain, between 2014 and 2018. Just over one in four (27 patients; 27.5%) of the 98 patients treated with immunotherapy agents over this four-year period were aged 70 years or older. PD-L1 status was known in 50% of patients.
Overall survival in these elderly patients was significantly shorter than in patients younger than 70 years of age (median 5.5 months vs 13 months, hazard ratio [HR] 3.86, 95% confidence interval [CI] 2.073-7.214, p
Considering toxicity, there were no statistically significant differences in immune-related adverse events between elderly and younger patients (p=0.535).
The study shows that immunotherapy was administered mainly as second-line treatment (61% of patients) or third-line or later (24.5%) across the entire group of 98 patients of all ages. Just over half (52%) were treated with nivolumab.
“Our results suggest that elderly patients could have worse survival outcomes with immunotherapy than younger patients, without differences in terms of toxicity,” said study authors Elena Corral de la Fuente and Arantzazu Barquin Garcia, from the Hospital Universitario Ramon y Cajal, Madrid, Spain. They acknowledged that the study was limited by being an observational retrospective analysis with a small sample size. They suggested, “Prospective randomised clinical trials and more real-world data are needed to answer remaining questions on the use of immunotherapy in elderly patients.”
Pooled analysis demonstrates improved overall survival with immunotherapy
A second study pooling data from three randomised trials (2) shows significantly improved overall survival in elderly patients with advanced NSCLC treated with the immunotherapy agent pembrolizumab compared to those given chemotherapy.
The study compared the efficacy and safety results for 264 elderly patients aged greater than or equal to 75 years in the three trials with results for 2292 participants younger than 75 years. All of the patients had PD-L1 tumour proportion scores (PD-L1 TPS) of 1% or higher and half of the elderly group in this analysis had scores of at least 50% (5).
Results show significantly improved overall survival in elderly patients with PD-L1 tumours scores greater than or equal to 1% treated with pembrolizumab compared to those treated with chemotherapy (hazard ratio [HR] 0.76, 95% confidence interval [CI] 0.56-1.02). The improvement in overall survival with pembrolizumab compared to chemotherapy was even greater in patients with PD-L1 tumour scores greater than or equal to 50% (HR 0.41, 95% CI 0.23-0.73).
One-year overall survival rates with pembrolizumab in elderly patients were comparable to those in younger patients (53.7% vs 54.9% in PD-L1 TPS greater than or equal to 1% and 61.7% vs 61.7% in PD-L1 TPS greater than or equal to 50%).
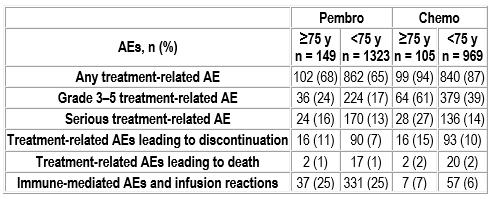
Fewer elderly patients treated with pembrolizumab had treatment-related adverse events compared to those treated with chemotherapy (68% vs 94%). Grade 3-5 treatment-related adverse events in elderly patients were also less common with pembrolizumab compared to chemotherapy (24% vs 61%). Common treatment-related adverse events with pembrolizumab in elderly patients were fatigue (17.4%), decreased appetite (12.8%) and pruritus (12.8%).
Immune-mediated adverse events and infusion reactions were more frequent with pembrolizumab vs chemotherapy in the elderly group of patients (25% vs 7%) but showed no difference compared to younger patients treated with pembrolizumab (25%).
“In elderly patients with advanced NSCLC with PD-L1-positive tumours, pembrolizumab monotherapy improved overall survival over chemotherapy, together with a more favourable safety profile,” said lead author Kaname Nosaki, from the National Hospital Organization Kyushu Cancer Center, Fukuoka, Japan. He added, “Our data support the use of pembrolizumab monotherapy in elderly patients (greater than or equal to 75 years) with advanced PD-L1- expressing NSCLC.”
Considering potential limitations, Nosaki noted that the elderly patients included in the pooled analysis met the inclusion criteria for each of the individual studies, which would have selected for a relatively fit elderly patient population.
Commenting on the studies, Marina Garassino, Chief of Thoracic Oncology at the Istituto Nazionale dei Tumori, Milan, Italy, said, “The pooled analysis of clinical trials showed no difference in the efficacy and safety of immunotherapy in the elderly compared to younger patients. But the real-world study is an alarm bell potentially suggesting lower efficacy with immunotherapy in elderly patients despite no difference in adverse events.” In terms of limitations, she noted that PL-1 expression was known in only 50% of patients included in the real-world study and that data were collected retrospectively. “Data collected in real-world studies are not controlled as precisely as in randomised trials,” she noted, but added that elderly patients are generally under-represented in clinical trials.
Looking to the future, Garassino concluded, “We need larger, prospective trials or larger real-world studies to gain a more detailed view on the efficacy and safety of immunotherapy in elderly patients with NSCLC.”
###
Notes to Editors
Please make sure to use the official name of the meeting in your reports: European Lung Cancer Congress (ELCC) 2019
Official Congress hashtag: #ELCC19
Disclaimer
This press release contains information provided by the authors of the highlighted abstract and reflects the content of this abstract. It does not necessarily reflect the views or opinions of ESMO or IASLC who cannot be held responsible for the accuracy of the data. Commentators quoted in the press release are required to comply with the ESMO Declaration of Interests policy and the ESMO Code of Conduct.
References
1 Abstract 169P_PR ‘Benefit of immunotherapy (IT) in advanced non-small cell lung cancer (NSCLC) in elderly patients (EP)’ will be presented by Elena Corral de la Fuente during the Poster Display Session on Thursday, 11 April 2019, 12:30 (CEST) in Hall 1. Annals of Oncology, Volume 30, 20019 Supplement 2. doi:10.1093/annonc/mdz072
2 Abstract 103O ‘Safety and efficacy of pembrolizumab (Pembro) monotherapy in elderly patients (Pts) with PD-L1-positive advanced NSCLC: Pooled analysis from KEYNOTE-010, -024 and -042’ will be presented by Kaname Nosaki during the ESMO-IASLC Best Abstracts Session on Thursday, 11 April 2019, 14:45 (CEST) in Room B. Annals of Oncology, Volume 30, 20019 Supplement 2. doi:10.1093/annonc/mdz072
The pembrolizumab study pooled results from three randomised, controlled trials:
* KEYNOTE-010 included patients with advanced NSCLC and PD-L1 tumour proportion score greater than or equal to 1%. Patients were randomised to pembrolizumab (2 or 10mg/kg once every three weeks)
or docetaxel, as second- or later-line therapy.
* KEYNOTE-042 also included patients with advanced NSCLC and PD-L1 tumour proportion score greater than or equal to 1%. Patients were random-ised to first-line pembrolizumab (200mg/kg once every three weeks) or platinum-based chemotherapy.
* KEYNOTE-024 included patients with advanced NSCLC and PD-L1 tumour proportion score greater than or equal to 50%. Patients were randomised to first-line pembrolizumab (200mg/kg once every three weeks) or platinum-based chemotherapy.
3 Planchard D, Popat S, Kerr K et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology 2018; 29 (supplement 4); iv192-iv237.
4 Pallis AG, Gridelli C, Wedding U et al. Management of elderly patients with NSCLC; updated expert’s opinion paper: EORTC Elderly Task Force, Lung Cancer Group and International Society for Geriatric Oncology. Annals of Oncology 2014; 25: 1270-1283.
5 PD-L1 TPS measures the proportion of tumour cells expressing PD-L1 (programmed-death ligand 1), which is the main ligand for the key immune checkpoint inhibitory receptor PD-1. A PD-L1 score of greater than or equal to1% means that at least 1% of tumour cells express PD-L1, while a PD-L1 score of greater than or equal to 50% indicates high PD-L1 expression, with at least 50% of tumour cells expressing PD-L1.
About the European Society for Medical Oncology (ESMO)
ESMO is the leading professional organisation for medical oncology. With more than 20,000 members representing oncology professionals from over 150 countries worldwide, ESMO is the society of reference for oncology education and information. ESMO is committed to offer the best care to people with cancer, through fostering integrated cancer care, supporting oncologists in their professional development, and advocating for sustainable cancer care worldwide. Visit http://www.
About the International Association for the Study of Lung Cancer (IASLC)
The International Association for the Study of Lung Cancer (IASLC) is the only global organisation dedicated solely to the study of lung cancer and other thoracic malignancies. Founded in 1974, the association’s membership includes more than 6,500 lung cancer specialists across all disciplines in over 100 countries, forming a global network working together to conquer lung and thoracic cancers worldwide. The association also publishes the Journal of Thoracic Oncology, the primary educational and informational publication for topics relevant to the prevention, detection, diagnosis and treatment of all thoracic malignancies. Visit http://www.
103O_PR – Safety and efficacy of pembrolizumab (Pembro) monotherapy in elderly patients (Pts) with PD-L1-positive advanced NSCLC: Pooled analysis from KEYNOTE-010, -024, and -042
K. Nosaki1, Y. Hosomi2, H. Saka3, P. Baas4, G. de Castro Jr5, M. Reck6, Y-L. Wu7, J.R. Brahmer8, E. Felip9, T. Sawada10, K. Noguchi10, S.R. Han10, B. Piperdi11, D.A. Kush11, G. Lopes12
1National Hospital Organization Kyushu Cancer Center, Fukuoka, Japan, 2Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome Hospital, Tokyo, Japan, 3National Hospital Organization Nagoya Medical Center, Nagoya, Japan, 4The Netherlands Cancer Institute and The Academic Medical Hospital Amsterdam, Amsterdam, Netherlands, 5Instituto do Cancer do Estado de Sao Paulo, Sao Paulo, Brazil, 6Lung Clinic Grosshansdorf, Airway Research Center North (ARCN), German Center for Lung Research (DZL), Grosshansdorf, Germany, 7Guangdong Lung Cancer Institute, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangdong, China, 8Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD, USA, 9Vall d’Hebron University Hospital, Barcelona, Spain, 10MSD K.K., Tokyo, Japan, 11Merck & Co., Inc., Kenilworth, NJ, USA, 12Sylvester Comprehensive Cancer Center at the University of Miami, Miami, FL, USA
Background: Approximately 70% of newly-diagnosed NSCLC cases occur in the elderly, and more than half are locally advanced/metastatic. We present a pooled analysis of efficacy and safety in elderly pts (aged greater than or equal to 75 y) enrolled in 3 randomized controlled trials of pembro monotherapy vs standard chemotherapy (chemo) for PD-L1-positive advanced NSCLC.
Methods: Pts were aged greater than or equal to 18 y with advanced NSCLC with PD-L1 tumor proportion score (TPS) greater than or equal to 1% (KEYNOTE-010, -042) or TPS greater than or equal to 50% (KEYNOTE-024). In KEYNOTE-010, pts were randomized to pembro 2 or 10 mg/kg Q3W or docetaxel, as second- or later-line therapy. In KEYNOTE-024 and -042, pts were randomized to first-line pembro 200 mg Q3W or platinum-based chemo. OS was estimated by the Kaplan-Meier method.
Results: The 3 trials included 264 pts aged greater than or equal to 75 (range, 75-90) y with TPS greater than or equal to 1%; 132 pts had TPS greater than or equal to 50%. Independent of line of treatment, HRs (95% CI) for OS favored pembro vs chemo: 0.76 (0.56-1.02) in pts with TPS greater than or equal to 1% and 0.40 (0.25-0.64) in pts with TPS greater than or equal to 50%. Pembro also improved OS vs chemo in the pooled analysis of pts with TPS greater than or equal to 50% who received first-line therapy (KEYNOTE-024 and -042): HR, 0.41 (95% CI, 0.23-0.73). Overall, fewer treatment-related AEs across various categories were observed with pembro vs chemo, in particular, grade 3-5 treatment-related AEs in pts aged greater than or equal to 75 y (Table). Immune-mediated AEs and infusion reactions were more frequent with pembro vs chemo, with similar frequency in pts receiving pembro aged greater than or equal to 75 y and
Conclusions: In this pooled analysis of pts aged greater than or equal to 75 y with PD-L1-positive advanced NSCLC, pembro monotherapy improved OS vs chemo, both in pts with PD-L1 TPS greater than or equal to 1% and PD-L1 TPS greater than or equal to 50%. The safety profile of pembro was similar in pts aged greater than or equal to 75 y and
Clinical trial identification: NCT01905657 (KEYNOTE-010); NCT02142738 (KEYNOTE-024); NCT02220894 (KEYNOTE-042)
Editorial acknowledgement: Medical writing and editorial assistance was provided by Michael S. McNamara, MS, of C4 MedSolutions, LLC (Yardley, PA), a CHC Group company. This assistance was funded by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA.
Legal entity responsible for the study: Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA
Funding: This research was supported by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA.
Disclosure: K. Nosaki: Honoraria: AstraZeneca, Chugai Pharmaceutical, Eli Lilly, MSD; Institutional research funding: MSD.
Y. Hosomi: Personal fees: MSD, AstraZeneca, Eli Lilly Japan, Taiho Pharmaceutical, Chugai Pharmaceutical, Ono Pharmaceutical, Bristol-Myers Squibb.
H. Saka: Grants/research support: AstraZeneca, MSD, Ono Pharmaceutical; Honoraria: AstraZeneca, MSD, Ono Pharmaceutical, Chugai Pharmaceutical, Boehringer Ingelheim, Kyorin Pharmaceutical.
P. Baas: Consulting role: Genentech/Roche, Merck, Bristol-Myers Squibb, Pfizer; Research support: Bristol-Myers Squibb, Roche, Merck.
G. de Castro Jr: Consulting/advisory role: AstraZeneca, MSD, BMS, Roche, Novartis, Boehringer Ingelheim; Speakers’ bureau: MSD, BMS, Novartis, AstraZeneca; Travel/accommodation expenses: MSD, BMS, Roche, Bayer, Novartis, Boehringer Ingelheim, AstraZeneca.
M. Reck: Personal fees: Amgen, Hoffmann-La Roche, Lilly, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, MSD, Merck, Novartis, Pfizer, AbbVie.
Y-L. Wu: Honoraria: AstraZeneca, Eli Lilly, Roche, Pierre Fabre, Pfizer, Sanofi; Consulting/advisory role: AstraZeneca, Roche, Merck, Boehringer Ingelheim; Research funding to institution: Boehringer Ingelheim, Roche.
J.R. Brahmer: Grant, personal fees, Advisory boards, consulting: Merck; Uncompensated advisor and consultant: Bristol-Myers Squibb; Grants: Bristol-Myers Squibb, MedImmune/AstraZeneca; Personal fees: Amgen, Celgene, Lilly.
E. Felip: Consulting, advisory role, speaker’s bureau: AbbVie, AstraZeneca, Blueprint Medicines, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Guardant Health, Janssen, Merck KGaA, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Takeda; Research funding: Fundación Merck Salud; Grant for Oncology Innovation EMD Serono.
T. Sawada, K. Noguchi, S.R. Han: Employee: MSD K.K., Tokyo, Japan.
B. Piperdi, D.A. Kush: Employee of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA.
G. Lopes: Research funding to institution: Merck & Co., Inc., EMD Serono, AstraZeneca.
169P_PR – Benefit of immunotherapy (IT) in advanced non-small cell lung cancer (NSCLC) in elderly patients (EP)
E. Corral de la Fuente1, A. Barquin Garcia2, C. Saavedra Serrano3, M.E. Olmedo Garcia3, R. Martin Huertas2, J.J. Serrano Domingo2, V. Albarran Artahona2, A. Gomez Rueda3
1Oncology, Hospital Universitario Ramon y Cajal, Madrid, Spain, 2Hospital Universitario Ramon y Cajal, Madrid, Spain, 3Medical Oncology, Hospital Universitario Ramon y Cajal, Madrid, Spain
Background: Despite EP (aged greater than or equal to 70 years) represent the majority of patients with advanced NSCLC, the efficacy and toxicity rates of IT remain poorly described, as they are under-represented in clinical trials. Furthermore, the age-related decline in the immune system might affect efficacy of IT.
Methods: We retrospectively reviewed advanced NSCLC patients treated with IT (antiPD-1, anti-PD-L1) monotherapy as first, second and subsequent-line settings, between 2014 and 2018 in our hospital. Patient and tumor features, irAEs, concomitant and subsequent treatments were collected. Stata 14.1 was used for the analysis.
Results: 98 patients were included. Mean age was 62 years (41-85). 73.5% were men. 73.5% had >30 smoked pack-years (py), 64.3% were adenocarcinoma (ADC), of which 41% were KRAS mutated; and 25.5% were squamous (SCC). PDL1 was known in a 50% of patients (11% 50%). IT was administered mainly as a second line (61%) and third or later (24.5%). Most employed drug was nivolumab (52%) (Table1). Response Rate (RR) was 32.7% (partial response 28%, complete response 5%). Disease control rate (DCR) was 55%. Overall Survival (OS) was significantly lower in EP compared to patients aged
Conclusions: Our results suggest that EP could have worse survival outcomes than younger patients, without differences in terms of toxicity, but prospective trials are needed to confirm this hypothesis.
Legal entity responsible for the study: Elena Corral de la Fuente
Funding: Has not received any funding
Disclosure: All authors have declared no conflicts of interest.
Media Contact
ELCC Press Office
[email protected]
Original Source
http://esmo.



{kind=link}