NHGRI-funded ClinGen panel also validates three genes believed to be associated with long QT syndrome
Credit: Darryl Leja, NHGRI
Geneticists and heart specialists around the world had previously reported 17 genes to cause long QT syndrome, a little-known inherited heart condition. However, the Clinical Genome Resource’s (ClinGen) expert panel has critically reevaluated the scientific evidence for all 17 reported genes, disputing nine of the genes and revealing only three of the genes to be definitively associated with the most common form of the disease. The work was funded by the National Human Genome Research Institute (NHGRI), part of the National Institutes of Health.
ClinGen is an NHGRI-funded resource that defines the clinical relevance or validity of genes in various genetic disorders for their use in precision medicine and research. Nine other genes have been classified as having limited or disputed evidence for causing the syndrome. Their results were published in Circulation, the peer-reviewed journal of The American Heart Association.
Normal hearts, abnormal rhythms
Twenty years ago, The New York Times published an article about three “apparently healthy” young people who died in seemingly mysterious ways, while sleeping, swimming and after playing soccer. In 2019, about 4,000 children and young adults died in the United States in similar, unusual ways. The apparent cause was long QT syndrome.
Long QT syndrome is caused by mutations in genes that regulate the heart’s electrical activity. These mutations can cause the heart to have sudden, irregular heart rhythms, or arrhythmias. Much like the cases in the New York Times article, people with long QT syndrome can have arrythmias that are both unprovoked or a result of stress and exercise. But when the arrythmias do occur, they can be fatal.
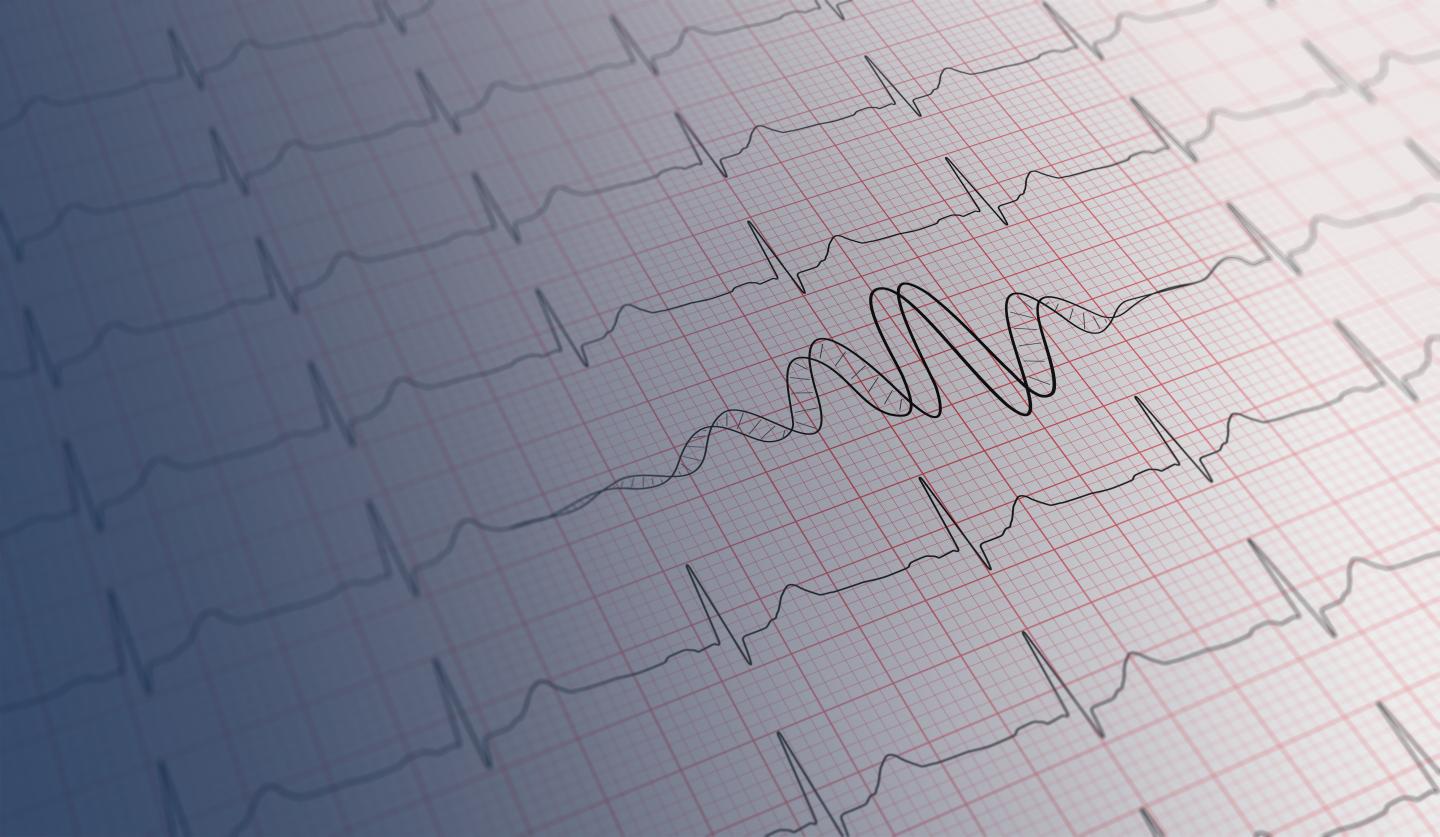
Many people with long QT syndrome may be unaware they have the condition, unless they get an unrelated electrocardiogram, know their family history and have undergone genetic testing. The term “QT” refers to the segment of an electrocardiogram which measures the duration of time for the heart to relax after a heartbeat. In long QT syndrome, that duration of time is abnormally prolonged and creates a vulnerability to dangerous arrhythmias.
Ever since the syndrome was described in 1957, researchers have engaged in a genetic race to identify the genes associated with long QT syndrome, which currently includes 17 genes.
By using such a standardized, evidence-based framework, the international ClinGen panel experts on long QT syndrome were able to classify the 17 genes into specific groups.
Three genes, KCNQ1, KCNH2 and SCN5A, had sufficient evidence to be implicated as “definitive” genetic causes for typical long QT syndrome. Four other genes had strong or definitive evidence supporting their role in causing atypical forms of long QT syndrome, presenting in the newborn period with associated heart block, seizures or delays in development. The remaining ten genes did not have sufficient evidence to support a causal role in the syndrome. In fact, nine of these 10 remaining genes were placed in the limited or disputed category. The study authors suggest that these genes not be routinely tested in clinical settings when evaluating patients and families with long QT syndrome, because they lack sufficient scientific evidence for causing for this condition.
ClinGen as an essential resource in precision medicine
Genetic testing providers use research papers to determine which genes to include in their testing panels for diagnostic reporting to physicians. Published papers reporting gene-disease associations vary widely in their study design and strength of evidence to support their conclusions. Until recently, standard guidelines that can differentiate between genes found with strong and valid scientific approaches versus those with insufficient evidence did not exist.
NHGRI developed the ClinGen resource to address this very issue.
ClinGen’s expert panels include researchers, clinicians and genetic counselors who apply an evidence-based framework in evaluating the scientific evidence from research papers to place gene-disease relationships into “definitive,” “strong,” “moderate,” “limited,” “disputed” or “refuted” categories.
“ClinGen is an impressive community effort. With over 1,000 researchers and clinicians from 30 countries volunteering their time and expertise, ClinGen is providing much needed clarity for the clinical genomics community regarding which gene-disease pairs have sufficient evidence to be used clinically,” said Erin Ramos, Ph.D., project scientist for ClinGen and program director in the Division of Genomic Medicine at NHGRI.
Clinical utility
“Our study highlights the need to take a step back and to critically evaluate the level of evidence for all reported gene-disease associations, especially when applying genetic testing for diagnostic purposes in our patients. Testing genes with insufficient evidence to support disease causation only creates a risk of inappropriately interpreting the genetic information and leading to patient harm,” says Michael Gollob, M.D., senior author of the paper and researcher at the Toronto General Hospital Research Institute.
Moreover, testing for genes not definitively associated with long QT syndrome can result in inappropriate and costly medical interventions such as implanting of a cardioverter-defibrillator, a heart device that can correct dangerous arrhythmias.
ClinGen researchers published a similar study in 2018, covering another heart condition called Brugada syndrome. In 2019, the American Society of Human Genetics considered the paper as one of the top 10 advances in genomic medicine.
With over 20 expert panels working on different diseases — breast and ovarian cancer, glaucoma and familial hypercholesterolemia to name a few — periodic classification of a number of gene-disease pairs is aimed to accelerate development of reliable and useful genetic tests over time.
###
Media Contact
Prabarna Ganguly
[email protected]
845-853-9910


{kind=link}