
Hilar cholangiocarcinoma (HCCA), recognized as the most prevalent malignant tumor within the biliary tract, presents a significant challenge in surgical oncology, with an alarming global incidence rate of 4.8 cases per 100,000 individuals annually. The stark survival statistics paint a concerning picture, showing a mere 20% to 50% 5-year overall survival rate among affected patients. As medical science progresses, various treatment modalities have been explored, but surgical resection remains a cornerstone of HCCA management. A contentious aspect of this surgical approach is the resection of the caudate lobe of the liver, an intervention that has sparked vigorous debate among oncological experts.
Historically, the practice of routinely performing caudate lobectomy has gained traction primarily due to the compelling observations made by Japanese research teams, which indicated that such procedures improved rates of negative surgical margins and localized recurrence. Aimless research from the United States and Europe corroborated these findings through retrospective analyses, thereby reinforcing the paradigm shift towards the standard operation of caudate lobe resection in surgical circles. Despite these trends, the scientific community has been hesitant due to a notable lack of robust evidence to substantiate these claims, making a thorough investigation vital.
A number of pivotal shortcomings have tainted the existing body of literature surrounding caudate lobe resection. Notably, selection bias looms large, as many studies have failed to rigorously define the surgical criteria that dictate the necessity for removing or retaining the caudate lobe. Consequently, surgical decisions often emerge from subjective interpretations made by individual surgeons, introducing unwanted variances that compromise the validity of research outcomes. Biased selection has rendered the reliability of existing studies questionable, necessitating a more comprehensive approach.
Methodological flaws further plague previous investigations, with a majority being retrospective in nature. The absence of Propensity Score Matching (PSM) to adjust for confounding variables generates considerable obstacles in accurately appraising the real effects of caudate lobectomy on surgical outcomes. Additionally, the primary objectives of most studies have been ambiguous, frequently lacking a clear focus on the direct consequences of caudate lobectomy on survival outcomes post-surgery.
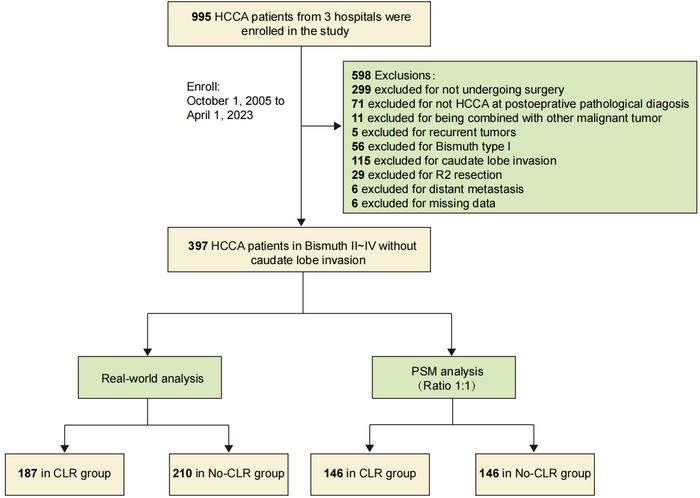
Addressing these concerns, a robust multicenter retrospective study was undertaken by a dedicated research team, aiming to shed light on these pressing issues. The analysis included 397 patients who underwent radical surgical resection for hilar cholangiocarcinoma across three leading medical centers in China from October 2005 to April 2023. For this pivotal study, only patients exhibiting no evidence of tumor invasion in the caudate lobe were recruited, either preoperatively or intraoperatively. Employing PSM allowed for a clear delineation between subjects who underwent caudate lobe resection and those who did not, facilitating a more accurate evaluation of surgical outcomes.
The findings of this rigorous investigation were enlightening. Remarkably, the study demonstrated that the rate of achieving R0 surgical margins in patients who underwent caudate lobe resection (CLR group) was significantly higher than in their non-resected counterparts (No-CLR group), with rates of 88.4% versus 76.0% respectively, supported by a p-value of 0.009. Despite this notable difference in margin achievement, a deeper analysis revealed no significant discrepancies in overall survival (OS) or recurrence-free survival (RFS) between the two cohorts, even after employing PSM. This unexpected result casts doubt on the perceived benefits of routine caudate lobe removal in improving long-term patient survival and recurrence rates.
The study’s supplementary subgroup analyses revealed compelling insights. It appeared that regardless of the status of caudate lobe resection, patients who achieved R0 margins fared better than those with R1 margins, a striking implication that resection status alone should not overshadow the critical nature of achieving a clear surgical margin. This pivotal evidence reiterates the significance of surgical margin status, suggesting that mere resection of the caudate lobe does not inherently confer survival advantages.
Diving deeper into multivariate analyses, a series of independent risk factors emerged. Increased preoperative CA19-9 levels and lower degrees of tumor differentiation surfaced as predictors of poorer OS, while adjuvant therapies demonstrated positive correlations with improved survival outcomes. Similarly, lower degrees of tumor differentiation and N2 staging emerged as determinants of RFS. These findings underscore the inherent biological behavior of tumors, suggesting that tumor characteristics play a pivotal role in shaping prognostic outcomes, and notably, CLR was not identified as an independent risk factor influencing postoperative survival.
For patients with HCCA who are confirmed to have no tumor invasion in the caudate lobe, the potential advantages of undertaking routine CLR include increased probabilities of achieving negative margins. Nonetheless, these potential benefits do not translate into clinical significance for RFS and OS, prompting a reevaluation of the role of caudate lobe resection in surgical practice, especially given the possibility of heightened incidence of mild complications.
This critical study offers invaluable insight into the surgical management of HCCA, pressing the need for surgeons to meticulously balance the pros and cons when faced with the decision to excise the caudate lobe in patients deemed free of tumors. In doing so, the research highlights the necessity of appreciating the biological characteristics manifest within tumors, emphasizing thoughtful consideration in postoperative adjuvant therapy while steering surgery towards more individualized and accurate treatment methodologies.
As the field advances, prospective randomized controlled trials with enhanced methodological rigor and expansive cohorts are essential for delineating the optimal strategies regarding the application of conventional caudate lobe resection in the treatment realm of HCCA. Only through such thorough investigation can we aspire to refine surgical paradigms and ultimately improve patient outcomes in the face of this formidable malignancy.
Subject of Research: Surgical management of hilar cholangiocarcinoma with a focus on caudate lobe resection.
Article Title: The Impact of Caudate Lobe Resection on Outcomes in Hilar Cholangiocarcinoma: New Insights from a Multicenter Study.
News Publication Date: TBD
Web References: TBD
References: TBD
Image Credits: ©Science China Press
Keywords: Hilar Cholangiocarcinoma, Caudate Lobe Resection, Surgical Outcomes, Propensity Score Matching, Overall Survival, Recurrence-Free Survival, Tumor Biology.
Tags: biliary tract malignanciescaudate lobe resection benefitscaudate lobectomy outcomesevidence-based surgical interventionsglobal cholangiocarcinoma incidenceHilar cholangiocarcinoma treatment strategiesoncological surgical practicesretrospective analyses in cancer surgerysurgical margin significance in cancersurgical oncology challengessurgical resection in liver cancersurvival rates in HCCA patients



{kind=link}