Peer-reviewed / Literature review, opinion / People
Credit: Credit: The Lancet
Peer-reviewed / Literature review, opinion / People
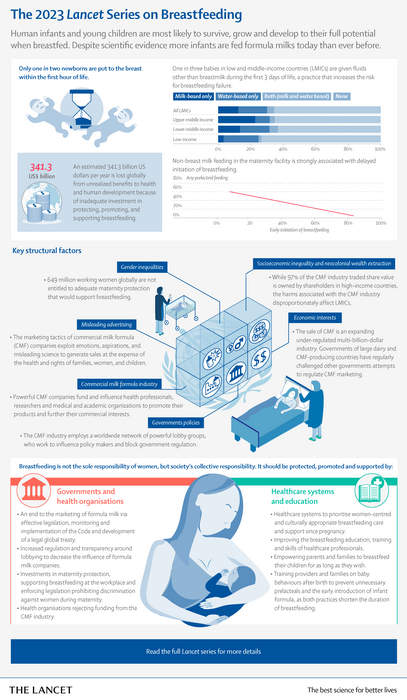
- Fewer than half of infants globally are breastfed as recommended by WHO [1], with formula milk sales on the rise despite formula feeding failing to offer the same nutrition, health and development benefits as breastfeeding.
- The Lancet 2023 Series on Breastfeeding argues that formula milk companies exploit parent’s emotions and manipulate scientific information to generate sales at the expense of the health and rights of families, women, and children.
- The Series highlights the economic and political power of the dominant formula milk companies and the public policy failures which mean millions of women are prevented from breastfeeding as recommended.
- The authors stress that breastfeeding is a collective responsibility of society and call for more effective promotion, support and protection for breastfeeding, including a much better trained healthcare workforce and an international legal treaty to end exploitative formula milk marketing and prohibit political lobbying.
Formula milk marketing tactics are exploitative, and regulations need to be urgently strengthened and properly implemented according to a new three paper Series publish in The Lancet. Experts call for an international legal treaty to end irresponsible formula milk marketing and political lobbying, accompanied by more effective breastfeeding support worldwide.
Series co-author, Professor Nigel Rollins, WHO, says “The sale of commercial milk formula is a multi-billion-dollar industry which uses political lobbying alongside a sophisticated and highly effective marketing playbook to turn the care and concern of parents and caregivers into a business opportunity. It is time for this to end. Women should be empowered to make choices about infant feeding which are informed by accurate information free from industry influence.”
He continues, “Our Series finds society, politics, and economics all contribute to why fewer than half of infants globally are breastfed as recommended [1]. Breastfeeding should be considered society’s collective responsibility, not the sole concern of women. We need to see wide-ranging actions across different areas of society to better support mothers to breastfeed for as long as they want.” [2]
“Babies are most likely to survive and grow to their full potential when breastfed. [3] Breastfeeding promotes brain development, protects infants against malnutrition, infectious diseases, and death, while also reducing risks of obesity and chronic diseases in later life. Yet, globally, many women who wish to breastfeed face multiple barriers, including insufficient parental leave and lack of support in healthcare systems and at the workplace, in the context of exploitative marketing tactics of the commercial milk formula industry”, says Series co-author Professor Rafael Pérez-Escamilla, Yale University School of Public Health, US. [2]
In a novel analysis, the Series describes how profits made by the formula milk industry benefit companies located in high-income countries while the social, economic and environmental harms are widely distributed and most harmful in low and middle income countries.
An exploitative marketing playbook
Triggered by The Baby Killer investigative report into Nestle’s marketing of formula milk in the Global South in the 1970s, the World Health Assembly developed the voluntary International Code of Marketing of Breast-milk Substitutes and subsequent resolutions (the Code) in 1981 [4]. However, the powerful influence of the milk formula industry and the marketing of their products in violation of the Code continues, with sales from commercial formula milk having rapidly increased over the past twenty years and now at more than $55 billion a year.
The Series outlines the exploitative tactics used by formula milk companies to sell their products, including taking advantage of parents’ worries about their child’s health and development. One common reason women introduce formula milk is interpretating unsettled baby behaviour, especially disrupted sleep and persistent crying, as a sign that breast milk is insufficient. [5,6] However, sleep patterns of babies are not the same as for adults and unsettled baby behaviours are common. When mothers are appropriately supported, concerns can be addressed successfully without the use of formula milk.
“The formula milk industry uses poor science to suggest, with little supporting evidence, that their products are solutions to common infant health and developmental challenges. Adverts claim specialised formulas alleviate fussiness, help with colic, prolong night-time sleep, and even encourage superior intelligence. Labels use words like ‘brain’, ‘neuro’ and ‘IQ’ with images highlighting early development, but studies show no benefit of these product ingredients on academic performance or long-term cognition. This marketing technique violates the 1981 Code, which says labels should not idealise the use of formula, and exploits poor science to create an untrue story to sell more product,” says Professor Linda Richter, Wits University, South Africa. [2] (For artwork illustrative of formula packaging see figure 3 and 4 in paper 2 of the Series. For a direct link to the images, please see notes to editors).
The Series explains how formula milk marketing exploits the lack of support for breastfeeding by governments and society to use gender politics to sell its products. The authors describe how the formula milk industry frames breastfeeding advocacy as a moralistic judgment that is anti-feminist and damaging to women, while presenting milk formula as a convenient and empowering solution for working mothers.
In recent years, digital communications have greatly increased the reach of marketing in ways that blur the difference between advertising and the provision of nutrition and care advice. The Series highlights examples of digital marketing such as industry-paid influencers sharing the difficulties of breastfeeding as preludes to formula milk marketing, and industry sponsored parenting apps with 24/7 chat services that enable product placement, offer free samples or deals, and promote online sales. The authors argue there is very little regulation of the formula milk industry online and there are regular violations of the Code.
A new review, conducted for the Series, of 153 studies details how marketing practices in violation of the Code have continued in nearly 100 countries and in every region of the world since its adoption more than forty years ago [7]. The Series says voluntary uptake of the Code is not enough and calls for an international legal treaty on the commercial marketing of food products for babies to protect the health and wellbeing of mothers and families.
The formula milk lobby
The Series also draws attention to the power of the milk formula industry to influence national political decisions and interfere with international and national regulatory processes. The formula industry has established a network of trade associations and front groups that lobby against the Code and other breastfeeding protection measures. For example, in 2012, South Africa passed new national legislation to implement The Code into law, however, this took nine years with many setbacks resulting from industry lobbying. Formula milk manufacturers formed a new lobby group, the Infant Feeding Association, which applied pressure for amendments to the regulations.
This outsourcing of lobbying allows the corporations themselves to project an image of benevolence and corporate social responsibility, suggesting that they can adequately self-regulate through corporate policies on responsible marketing. However, their self-regulation falls far short of compliance to the Code.
As well as influencing political organisations, the authors argue formula milk companies also draw on the credibility of science by sponsoring professional organisations, publishing sponsored articles in scientific journals, and inviting leaders in public health onto advisory boards and committees, leading to unacceptable conflicts of interest within public health.
“The voluntary Code is not working – formula milk companies chose to disregard the guidance and lobby at every opportunity to weaken regulation. We need a stricter international legal treaty on the marketing of milk formula which is incorporated into law across the world. The treaty must protect policymaking from industry influence, with obligations for senior public officials to divulge meetings with lobbyists and requirements for scientific organisations to disclose funding sources and members of expert advisory groups. This would regulate the commercial milk formula industry while not restricting the sale of the products to those who need or want them. More generally, the global and public health community must also be much more critical about public-private partnerships that enable or tolerate conflicts of interest” says Professor David McCoy. [2]
Society-wide changes needed
In addition to ending the marketing tactics and industry influence of formula milk companies, broader actions across workplaces, healthcare, governments, and communities are needed to more effectively support women who want to breastfeed.
Half a billion working women globally are not entitled to adequate maternity protection. A systematic review of studies found women with a minimum of three months maternity leave, paid or unpaid, were at least 50% more likely to continue breastfeeding compared to women returning to work within three months of giving birth [8]. The authors call for governments and workplaces to recognise the value of breastfeeding and care work, by actions such as extending paid maternity leave duration to align with the six month WHO recommended duration of exclusive breastfeeding.
Women also face a lack of breastfeeding promotion, protection and support within healthcare systems due to limited public budgets, skilled support by health workers, influence from milk formula industry and an absence of care that is culturally appropriate and led by the needs of women. Authors argue that breastfeeding outcomes improve when health systems actively empower women and enable experienced peers to support women during pregnancy, childbirth and onwards. Healthcare providers should offer skilled counselling before and after birth to all mothers to enable them to address unsettled baby behaviours whilst continuing to breastfeed if they wish to do so.
Sonia Hernández-Cordero, Universidad Iberoamericana, Mexico City says, “We are seeing improvements in some countries. A case study which we commissioned for the Series found that, despite lacking federally mandated paid maternity leave, the US continues to recognise an increasing number of Baby-Friendly [9] hospitals each year, and the National Supplemental Nutrition Program for Women, Infants and Children (WIC), which reaches half of annual births in the US, is increasingly providing breastfeeding counselling as it continues to support more women to choose breastfeeding.” [2]
“Many governments fail to protect mothers and children from unethical marketing practices because of the economic and political power of trans-national companies. The extreme power of corporations relative to public-interest bodies must be re-balanced. Anti-trust legislation and the ending of corporate tax abuse would help reverse the favouring of private financial interests at the expense of the rights of mothers and infants”, says Professor David McCoy, United Nations University. [2]
“Advice that breastfeeding is best for their babies’ health is no use if women are not supported to understand and manage unsettled baby behaviours, or if mothers without maternity leave or pay are forced to go back to work out of financial necessity”, says Dr Julie Smith, Australian National University. [2]
A large expansion in health professional training on breastfeeding, as well as statutory paid maternity leave and other protections are vital. This requires changing the way society views breastfeeding as the sole responsibility of individual women and putting the onus across all levels of society,” says Professor Rafael Pérez-Escamilla, Yale School of Public Health. [2]
A linked Editorial published in The Lancet says, “Some women choose not to breastfeed, or are unable to. Perceived pressure, or inability, to breastfeed—especially if it is at odds with a mother’s wishes—can have a detrimental effect on mental health, and systems should be in place to fully support all mothers in their choices. Women and families make decisions about infant feeding based on the information they receive, and a criticism of the CMF industry’s predatory marketing practices should not be interpreted as a criticism of women. All information that families receive on infant feeding must be accurate and independent of industry influence to ensure informed decision making.”
NOTES TO EDITORS
The Global Series launch is on Wednesday 8th February at 12:30 – 14:00 UK time. It will be livestreamed here.
This Series received funding from BMGF for the research but not to authors for their time or writing. For a full list of researchers see the three papers.
[1] UNICEF. Global database 2021. Available from: https://data.unicef.org/topic/nutrition/breastfeeding/
[2] Quote direct from author and cannot be found in the text of the Article.
[3] Victora CG, Bahl R, Barros AJ, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. The Lancet 2016; 387(10017): 475-90.
[4] https://www.who.int/publications/i/item/9241541601
[5] Vilar-Compte M, Pérez-Escamilla R, Orta-Aleman D, Cruz-Villalba V, Segura-Pérez S, Nyhan K, Richter LM. Impact of baby behaviour on caregiver’s infant feeding decisions during the first 6 months of life: A systematic review. Matern Child Nutr. 2022 May;18 Suppl 3(Suppl 3):e13345. doi: 10.1111/mcn.13345.
[6] Segura-Pérez S, Richter L, Rhodes EC, Hromi-Fiedler A, Vilar-Compte M, Adnew M, Nyhan K, Pérez-Escamilla R. Risk factors for self-reported insufficient milk during the first 6 months of life: A systematic review. Matern Child Nutr. 2022 May;18 Suppl 3(Suppl 3):e13353. doi: 10.1111/mcn.13353.
[7] Becker GE, Zambrano P, Ching C, et al. Global evidence of persistent violations of the International Code of Marketing of Breast-milk Substitutes: A systematic scoping review. Maternal & child nutrition 2022; 18(S3): e13335.
[8] Navarro-Rosenblatt D, Garmendia ML. Maternity Leave and Its Impact on Breastfeeding: A
Review of the Literature. Breastfeed Med 2018; 13(9): 589-97.
[9] https://www.unicef.org.uk/babyfriendly/
The labels have been added to this press release as part of a project run by the Academy of Medical Sciences seeking to improve the communication of evidence. For more information, please see: http://www.sciencemediacentre.org/wp-content/uploads/2018/01/AMS-press-release-labelling-system-GUIDANCE.pdf if you have any questions or feedback, please contact The Lancet press office [email protected]
IF YOU WISH TO PROVIDE A LINK FOR YOUR READERS, PLEASE USE THE FOLLOWING, WHICH WILL GO LIVE AT THE TIME THE EMBARGO LIFTS: www.thelancet.com/series/Breastfeeding-2023
Journal
The Lancet
Method of Research
Literature review
Subject of Research
People
Article Title
The Lancet 2023 Series on Breastfeeding
Article Publication Date
7-Feb-2023
COI Statement
Paper 1: NR received grants from the Bill & Melinda Gates Foundation during the
conduct of this study. All other authors declare no competing interests.
Paper 2: PB reports receiving funds from WHO to undertake research on the
political economy of infant and young child feeding, which included
research on CMF marketing. PB also reports funding from the Australian
Research Council, UNICEF, The World Bank, and WHO to undertake
research, prepare policy reviews, write reports, or attend meetings, outside
the submitted work. GK was employed by M&C Saatchi World Services,
which was commissioned by UNICEF and WHO to design and implement
a multicountry study examining the scope and influence of
CMF marketing. GH and DM report receiving funds from WHO to
undertake qualitative and secondary research on the political economy of
breastfeeding and other research describing the nature of CMF marketing.
KR reports receiving a research grant from Alive & Thrive and FHI360 that
supported earlier research that is now cited in this Series paper.
Paper 3: PB and DM report funding from the WHO Department of Maternal,
Newborn, Child and Adolescent Health and Ageing for conducting
reviews and specific analyses in preparation of this paper. All other
authors declare no competing interests. The findings reported in this
manuscript reflect the viewpoints and findings of the authors only,
and do not necessarily represent those of the study funder.

