Chief among the myriad practical updates to minimize risks for patients and imaging personnel alike is a tiered approach for delaying both outpatient and inpatient cross-sectional interventional procedures
Credit: American Journal of Roentgenology (AJR)
Leesburg, VA, June 3, 2020–An open-access article in the American Journal of Roentgenology (AJR) details myriad practical updates that radiologists performing cross-sectional interventional procedures should institute to minimize risks for patients and imaging personnel alike during the coronavirus disease (COVID-19) pandemic.
“Cross-sectional interventional procedures are performed under CT, ultrasound, fluoroscopy, or MRI guidance and include fluid aspiration, (thoracentesis, paracentesis, and fluid collections), drainage catheter placement, percutaneous biopsy, and tumor ablation,” explained lead author Ghaneh Fananapazir at the University of California Davis Medical Center.
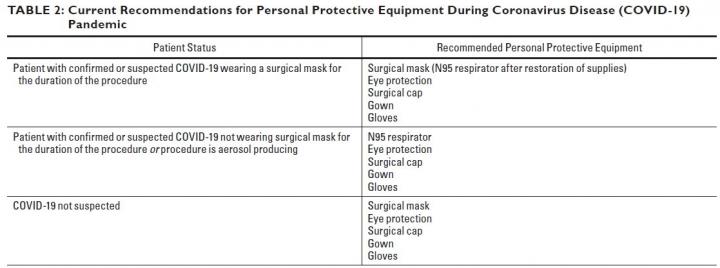
All of these procedures require appropriate donning and doffing of personal protective equipment by every member of the IR team–physician, trainee, nurse, technologist–and some procedures may require admitting the patient for management of postprocedure complications, necessitating a hospital bed and auxiliary resources.
Thus, for procedural delays that will not adversely affect patient outcome, Fananapazir and colleagues proposed the following tiered approach for both outpatient and inpatient scenarios: urgent procedures, procedures that should be performed within 2 weeks, procedures that should be performed within 2 months, and procedures that can safely be delayed 2 or 6 months.
“Each procedure request must be triaged into a tier on a case-by-case basis,” Fananapazir et al. warned, “because clinical circumstances can dictate one procedure as urgent, whereas different clinical data may render the same procedure safe to delay.” When considering any procedural delay, Fananapazir’s team strongly recommended consultation with the referring physician, who may have insights not available to the interventional radiologist.
Wherever possible, procedures should be performed bedside in COVID-19 units (or patient rooms, should no dedicated COVID-19 unit exist). Regarding ultrasound-guided procedures, specifically, a mobile ultrasound unit can be left in place in the ICU or the COVID-19 unit–“used for interventional procedures, guidance for vascular access, or point-of-care thoracic and nonthoracic ultrasound,” wrote Fananapazir et al. Ultrasound probes should be sterilized according to manufacturer guidelines.
Fananapazir’s team also cautioned against CT technologists or sonographers entering the procedure room. Ideally, all anticipated IT tray supplies should be acquired before the procedure commences, covered with a sterile plastic drape, and opened only to the extent needed.
Additionally, patient interaction during the informed consent interview can be limited by obtaining consent in the procedure room or using documented oral consent in the medical record. “Both of these modifications to the consent process are outside of standard regulated practice,” the authors of this AJR article noted, “therefore, establishment of hospital-wide frameworks may be needed.”
###
Founded in 1900, the American Roentgen Ray Society (ARRS) is the first and oldest radiological society in North America, dedicated to the advancement of medicine through the profession of radiology and its allied sciences. An international forum for progress in medical imaging since the discovery of the x-ray, ARRS maintains its mission of improving health through a community committed to advancing knowledge and skills with an annual scientific meeting, monthly publication of the peer-reviewed American Journal of Roentgenology (AJR), quarterly issues of InPractice magazine, AJR Live Webinars and Podcasts, topical symposia, print and online educational materials, as well as awarding scholarships via The Roentgen Fund®.
Media Contact
Logan K. Young
[email protected]
Original Source
https:/
Related Journal Article
http://dx.



{kind=link}