Credit: Antti Roine
An artificial nose developed at Tampere University, Finland, helps neurosurgeons to identify cancerous tissue during surgery and enables the more precise excision of tumours.
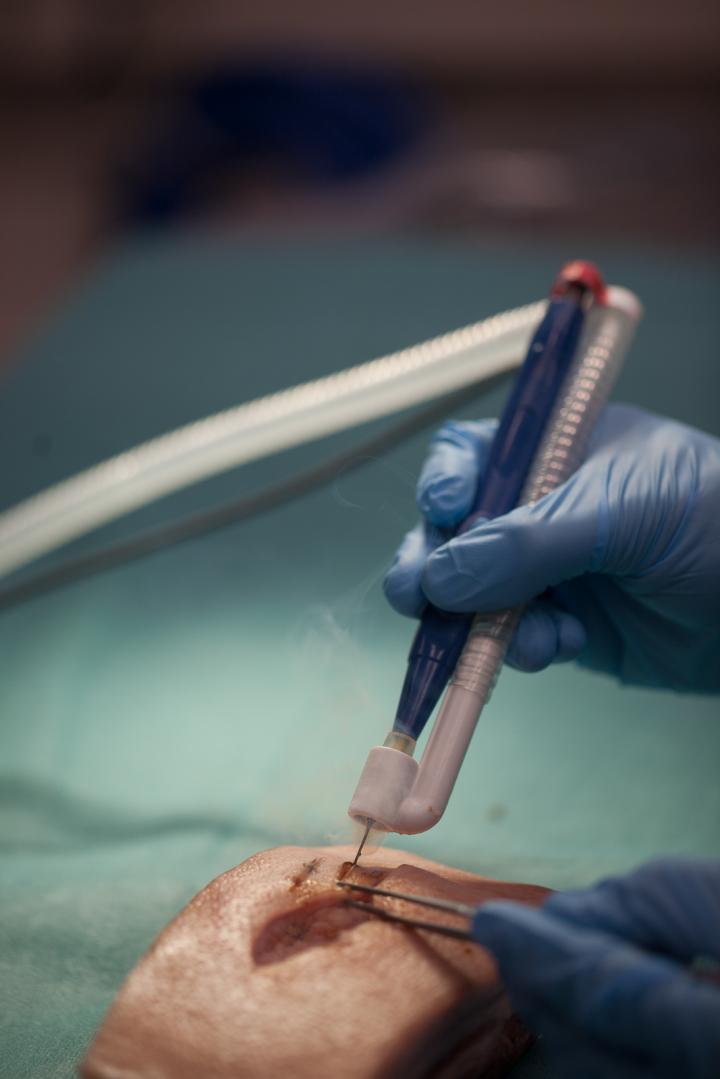
Electrosurgical resection using devices such as an electric knife or diathermy blade is currently a widely used technique in neurosurgery. When tissue is burned, tissue molecules are dispersed in the form of surgical smoke. In the method developed by researchers at Tampere University, the surgical smoke is fed into a new type of measuring system that can identify malignant tissue and distinguish it from healthy tissue.
An article on using surgical smoke to identify brain tumours was recently published in the Journal of Neurosurgery.
“In current clinical practice, frozen section analysis is the gold standard for intraoperative tumour identification. In that method, a small sample of the tumour is given to a pathologist during surgery,” says researcher Ilkka Haapala from Tampere University.
The pathologist undertakes a microscopic analysis of the sample and phones the operating theatre to report the results.
“Our new method offers both a promising way to identify malignant tissue in real time and the ability to study several samples from different points of the tumour,” Haapala explains.
“The specific advantage of the equipment is that it can be connected to the instrumentation already present in neurosurgical operating theatres,” Haapala points out.
The technology is based on differential mobility spectrometry (DMS), wherein flue gas ions are fed into an electric field. The distribution of ions in the electric field is tissue-specific, and the tissue can be identified on the basis of the resulting “odour fingerprint”.
The study analysed 694 tissue samples collected from 28 brain tumours and control specimens.
The equipment used was developed specifically for the study. It consists of a machine learning system, which analyses the flue gas with DMS technology, and an electric knife, which is used to produce the flue gas from the tissues.
The system’s classification accuracy was 83% when all the samples were analysed. The accuracy improved in more restricted settings. When comparing low malignancy tumours (gliomas) to control samples, the classification accuracy of the system was 94%, reaching to 97% sensitivity and 90% specificity.
###
Media Contact
Ilkka Haapala
[email protected]



{kind=link}