Credit: Rebholz
Highlight
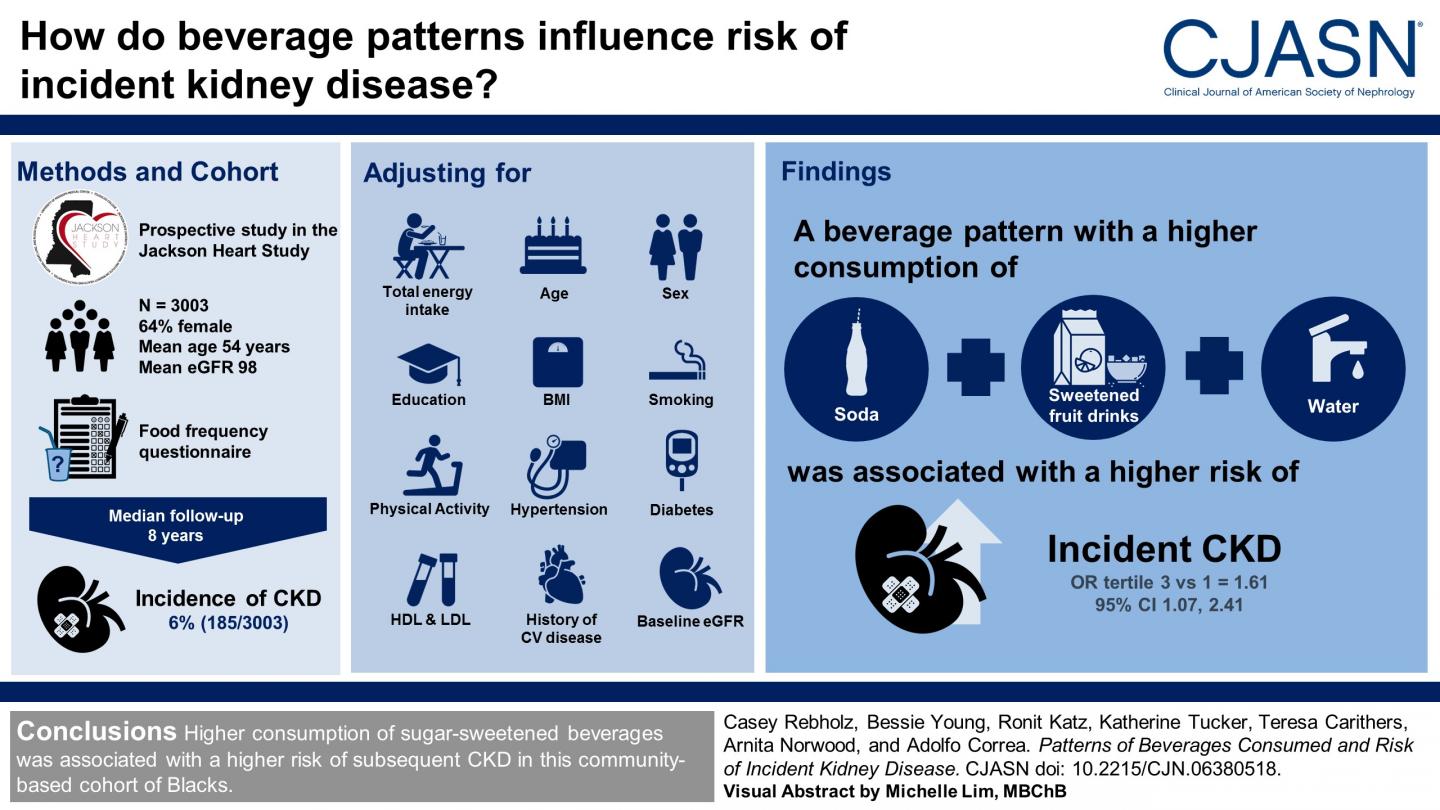
- In a study of African-American men and women with normal kidney function, a pattern of higher collective consumption of soda, sweetened fruit drinks, and water was associated with a higher risk of developing kidney disease.
Washington, DC (December 27, 2018) — Higher collective consumption of sweetened fruit drinks, soda, and water was associated with a higher likelihood of developing chronic kidney disease (CKD) in a community-based study of African-American adults in Mississippi. The findings, which appear in an upcoming issue of the Clinical Journal of the American Society of Nephrology (CJASN), contribute to the growing body of evidence pointing to the negative health consequences of consuming sugar-sweetened beverages.
Certain beverages may affect kidney health, but study results have been inconsistent. To provide more clarity, Casey Rebholz PhD, MS, MNSP, MPH (Johns Hopkins Bloomberg School of Public Health) and her colleagues prospectively studied 3003 African-American men and women with normal kidney function who were enrolled in the Jackson Heart Study.
“There is a lack of comprehensive information on the health implications of the wide range of beverage options that are available in the food supply,” said Dr. Rebholz. “In particular, there is limited information on which types of beverages and patterns of beverages are associated with kidney disease risk in particular.”
For their study, the investigators assessed beverage intake through a food frequency questionnaire administered at the start of the study in 2000-04, and they followed participants until 2009-13.
Among the 3003 participants, 185 (6%) developed CKD over a median follow-up of 8 years. After adjustment for confounding factors, consuming a beverage pattern consisting of soda, sweetened fruit drinks, and water was associated with a higher risk of developing CKD. Participants in the top tertile for consumption of this beverage pattern were 61% more likely to develop CKD than those in the bottom tertile.
The researchers were surprised to see that water was a component of this beverage pattern that was linked with a higher risk of CKD. They noted that study participants may have reported their consumption of a wide variety of types of water, including flavored and sweetened water. Unfortunately, the investigators did not collect information about specific brands or types of bottled water in the Jackson Heart Study.
In an accompanying editorial, Holly Kramer, MD, MPH and David Shoham, PhD (Loyola University Chicago) noted that the findings hold strong public health implications. “While a few select U.S. cities have successfully reduced SSB [sugar sweetened beverage] consumption via taxation, all other municipalities have resisted public health efforts to lower SSB consumption,” they wrote. “This cultural resistance to reducing SSB consumption can be compared to the cultural resistance to smoking cessation during the 1960s after the Surgeon General report was released. During the 1960s, tobacco use was viewed as a social choice and not a medical or social public health problem.”
In an accompanying Patient Voice editorial, Duane Sunwold explained that he is a patient with CKD who changed his eating and drinking patterns to put his disease in remission. As a chef, he offers a number of recommendations to fellow patients trying to decrease their consumption of sugar-sweetened drinks.
###
Study co-authors include Bessie Young, MD, MPH, Ronit Katz, PhD, Katherine Tucker, PhD, Teresa Carithers, PhD, RD, LD, Arnita Norwood, PhD, MPH, RD, and Adolfo Correa, MD, PhD, MPH.
Disclosures: The authors reported no financial disclosures.
The article, entitled “Patterns of Beverages Consumed and Risk of Incident Kidney Disease,” will appear online at http://cjasn.
The accompanying editorial, entitled “The Millennial Physician and the Obesity Epidemic: A Tale of Sugar Sweetened Beverages,” will appear online at http://cjasn.
The Patient Voice editorial, entitled “Diet and Risk for Developing Kidney Disease,” will appear online at http://cjasn.
The content of this article does not reflect the views or opinions of The American Society of Nephrology (ASN). Responsibility for the information and views expressed therein lies entirely with the author(s). ASN does not offer medical advice. All content in ASN publications is for informational purposes only, and is not intended to cover all possible uses, directions, precautions, drug interactions, or adverse effects. This content should not be used during a medical emergency or for the diagnosis or treatment of any medical condition. Please consult your doctor or other qualified health care provider if you have any questions about a medical condition, or before taking any drug, changing your diet or commencing or discontinuing any course of treatment. Do not ignore or delay obtaining professional medical advice because of information accessed through ASN. Call 911 or your doctor for all medical emergencies.
Since 1966, ASN has been leading the fight to prevent, treat, and cure kidney diseases throughout the world by educating health professionals and scientists, advancing research and innovation, communicating new knowledge, and advocating for the highest quality care for patients. ASN has more than 20,000 members representing 131 countries. For more information, please visit http://www.
Media Contact
Tracy Hampton
[email protected]
Related Journal Article
http://dx.


{kind=link}