Clinicians should carefully monitor patients treated with chloroquine therapy, particularly elderly women and others at higher risk for heart rhythm abnormalities, investigators caution in the journal Heart Rhythm
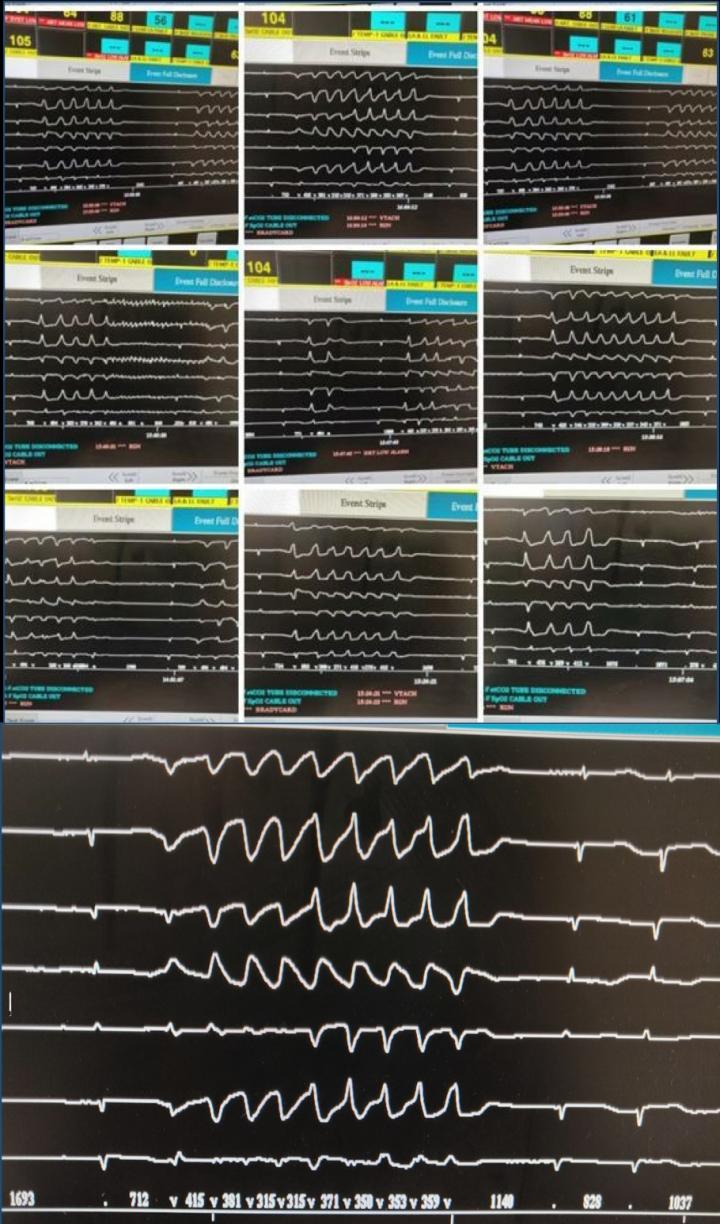
Credit: Heart Rhythm
Philadelphia, June 18, 2020 – A patient who met many of the published safety guidelines for chloroquine therapy against COVID-19 was observed to have a very abnormal ECG pattern after treatment began, leading to multiple episodes of torsade de pointes (TdP), a life-threatening arrhythmia in which the lower chambers of the heart beat out of sync with the upper chambers. Her condition was resolved after chloroquine was discontinued, investigators report in Heart Rhythm, the official journal of the Heart Rhythm Society, the Cardiac Electrophysiology Society, and the Pediatric & Congenital Electrophysiology Society, published by Elsevier.
Chloroquine and hydroxychloroquine are commonly used to treat malaria and some rheumatic diseases. Their use as a treatment for COVID-19 has been widely debated in medical journals and the popular press. The authors of this case report present the first description of TdP due to chloroquine treatment in a patient with COVID-19.
Lead investigator Yishay Szekely, MD, Department of Cardiology, Sourasky Tel Aviv Medical Center and Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel, observes, “On the one hand, these drugs are known to cause prolongation of a specific ECG interval called QT interval. On the other hand, there is no evidence of sudden, unexplained death when they are used to treat malaria. And by the same token, neither the American nor the European rheumatology societies recommend electrocardiographic (ECG) surveillance for patients who receive long-term treatment with hydroxychloroquine.”
The patient, an 84 year-old women with a history of breast cancer and controlled hypertension was admitted to the hospital with COVID-19. Her medications included letrozole, prescribed for breast cancer, and memantine, prescribed for Alzheimer’s disease. An ECG found her corrected QT (QTc) interval was 462 milliseconds, borderline high but still below the 500-millisecond limit suggested by safety guidelines for chloroquine treatment. Her condition worsened and chloroquine therapy was introduced. After five days of treatment, there was no change to her clinical status, however, a follow-up ECG showed signs of an extremely elongated QTc interval of 627 milliseconds. Chloroquine was discontinued, as were other drugs known or suspected of causing QT-prolongation, including memantine and letrozole.
The patient was placed on a continuous ECG monitor and given potassium supplements to prevent arrhythmias. Six hours later episodes of TdP were noted on her ECG. She received treatment that led to an immediate resolution of the ventricular arrhythmias, and her QT interval gradually normalized. She was released after two weeks.
Dr. Szekely notes that the memantine the patient was taking likely contributed to the proarrhythmic effects of chloroquine. However, her QTc interval spiked only after chloroquine was introduced. “This clearly points to chloroquine as the culprit drug of her TdP.” The breast cancer medication letrozole is actually considered safer from a QT interval point of view than other medications used to treat breast cancer.
“Chloroquine therapy is not free of risk in patients with COVID-19, particularly in those with high risk features for QT prolongation and TdP,” says Dr. Szekely. “Given its questionable efficacy in the treatment of COVID-19 and risk of QT interval prolongation and torsade de pointes, chloroquine treatment must be considered thoroughly and reviewed on a regular basis.”
###
Media Contact
Jane Grochowski
[email protected]
Related Journal Article
http://dx.



{kind=link}