
In a landmark case study published by Eurosurveillance, the emergence of a non-autochthonous Mycobacterium leprae infection in Ireland sheds light on critical issues within public health responses to rare diseases. The report details a multifaceted situation involving an adult case of leprosy, which has posed significant challenges due to the infrequency of this disease in a high-income country context, highlighting systemic gaps in healthcare protocols and resources available for rare infectious diseases.
Leprosy, an ancient ailment caused by Mycobacterium leprae, has historically been a public health concern primarily in developing regions. Despite being classified as one of the 24 neglected tropical diseases targeted for elimination by the World Health Organization, leprosy remains a significant burden globally, with over 180,000 reported cases. The recent detection of leprosy in Ireland, however, raises questions about the preparedness of medical professionals and the healthcare system to handle such rare instances effectively.
The diagnosed patient, an individual in their thirties, was originally from the Caribbean—a region where leprosy is still prevalent. They moved to Ireland two years before their diagnosis and presented with alarming neurological symptoms and skin lesions. This late diagnosis reveals systemic issues within healthcare systems, particularly concerning awareness and recognition of leprosy symptoms among professionals in regions where the disease is rare.
After an extensive seven-month diagnostic journey featuring skin biopsies, the patient was eventually correctly diagnosed and treated with a multi-drug therapy regimen. This successful treatment serves as a crucial reminder of the importance of timely medical intervention. However, it also translates to an underlying concern regarding the prolonged timeline for diagnosis, which illustrates a lack of awareness surrounding the disease in the healthcare framework prevalent in Ireland and certainly in other regions with limited leprosy cases.
Contact tracing is pivotal in controlling the spread of infectious diseases. In this case, the public health response relied heavily on WHO guidelines, highlighting a severe deficiency as Ireland lacks specific local guidelines for leprosy. The lack of tailored guidelines impacts the efficacy of contact tracing and the subsequent healthcare response to such rare incidents, a situation exacerbated by the considerable social stigma associated with leprosy.
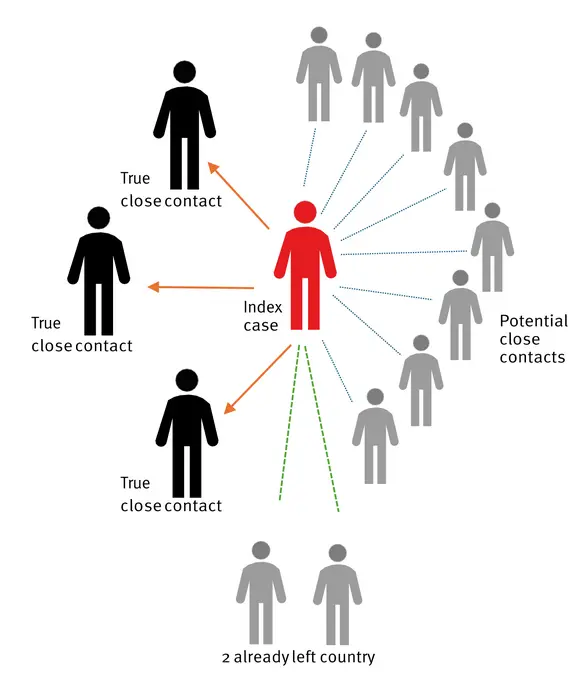
A comprehensive approach to outlining who qualifies as a close contact was adopted, defining close contact as individuals who had significant interactions with the initial patient. During this contact tracing process, it was discovered that one housemate, the patient’s partner, and a work-related acquaintance met the criteria for close contact under existing WHO definitions. Interestingly, ten additional adults were flagged as potential contacts, revealing the extensive network of people potentially affected, further complicating public health responses.
Stigmatization of leprosy sufferers, as revealed by the findings, led to a careful handling of the contact tracing strategy proposed by public health officials. Instead of contacting all household members, which might infringe on the patient’s social standing and housing security, targeted notifications respecting confidentiality and personal circumstances were pursued. This approach underscores a balancing act between ensuring public health safety and recognizing the human experience of those affected, revealing a multidimensional aspect of tackling disease in contemporary health settings.
Chemoprophylaxis with single-dose rifampicin was recommended for the three identified close contacts, as evidence supports its protective efficacy in regions where leprosy is endemic. However, the transference of such guidelines to high-income countries remains contentious. The lack of firm evidence regarding the effectiveness of such prophylactic treatments in low-incidence areas poses additional questions for healthcare policy-makers and practitioners.
The broad variability in leprosy’s incubation period—ranging from as short as two years to as long as twenty or more—presents further challenges in managing patient follow-up. International guidelines advocate for routine annual check-ups for close contacts spanning a minimum of five years, yet adherence to these recommendations in an Irish context highlights discrepancies in local public health strategies for monitoring and managing leprosy exposure.
In light of these findings, the study emphasizes essential recommendations for public health frameworks, particularly in areas where leprosy remains rare but conceivable. The case illuminates the necessity to equip healthcare professionals with targeted training focused on rare diseases, ongoing education, and the dispelling of myths surrounding leprosy to mitigate prevalent stigma.
The complexity of responding to rare diseases like leprosy in high-income countries indicates an urgent need for collaborative strategies that involve engaging healthcare professionals, policymakers, and affected individuals in dialogue that informs guidelines and practices tailored to specific contexts. Standardization across various public health guidelines is essential, thus improving response times and care outcomes for individuals presenting with atypical diseases.
The insights garnered from this case serve as a compelling reminder of the broader implications concerning neglected tropical diseases even in regions deemed high-income. These findings advocate for a proactive approach in public health that anticipates and addresses sporadic cases of diseases traditionally absent from local epidemiology while fostering a compassionate atmosphere for those affected.
The association between this single leprosy case and broader public health implications calls for increased governmental and institutional investment into health equity, creating robust systems that prioritize agency and reduce stigmatization for individuals afflicted by neglected tropical diseases. As countries work towards eliminating diseases like leprosy, comprehensive strategies supported by evidence-based guidelines remain critical in safeguarding public health.
By understanding the challenges and barriers faced in this specific case, health authorities can better allocate resources, improve training for healthcare providers, and foster an environment that prioritizes public health without compromising individual dignity. The emergence of such a case in an unexpected location underscores the continuing relevance of vigilance in surveillance efforts and the vital importance of education in combating infectious disease transmission in the global landscape.
Understanding the nuances inherent to this case enables health policymakers and professionals to confront the realities of illness, education, and stigma collaboratively. The case serves as a starting point for developing comprehensive public health strategies that reflect the complexities of managing rare diseases, ultimately striving for a more inclusive and aware healthcare system.
Subject of Research:
Article Title:
News Publication Date:
Web References:
References:
Image Credits:
Keywords: Leprosy, public health, neglected tropical diseases, epidemiology, contact tracing, chemoprophylaxis, health policy, stigma, infectious diseases, healthcare education, Mycobacterium leprae.


{kind=link}