In recent years, cholera has surged once again as a pressing global health threat, killing thousands and infecting hundreds of thousands annually. This resurgence has put governments and health organizations under immense pressure to devise more effective strategies to control outbreaks. Traditionally, antibiotic treatments for cholera have been narrowly reserved for only the most severe clinical cases, primarily to avoid accelerating the emergence of antibiotic-resistant bacterial strains. However, innovative mathematical modeling research from the University of Utah Health is now challenging this long-standing approach, suggesting that a broader application of antibiotics might paradoxically slow the spread of cholera while simultaneously lowering the risk of resistance development.
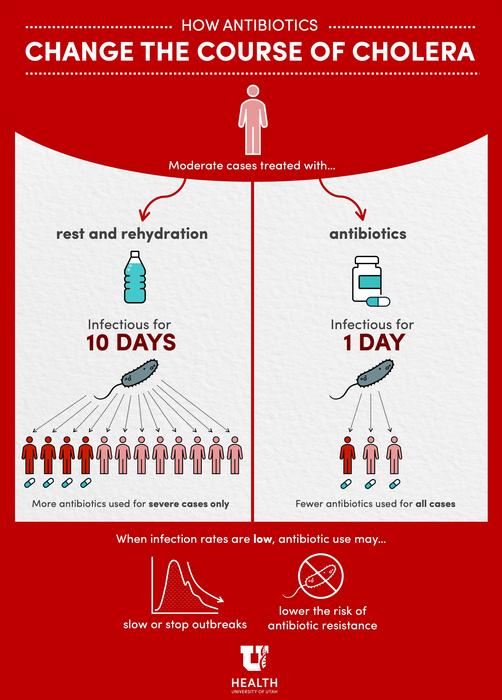
This groundbreaking research pivots on the understanding that antibiotics, beyond helping individual patients recover, significantly diminish the infectious period of cholera carriers. While current medical guidelines prioritize fluid rehydration and symptomatic care for mild and moderate infections, antibiotics reduce the time during which an infected individual sheds the bacterium into the environment by roughly tenfold. This reduction in infectiousness could have profound implications on community-level transmission dynamics, a notion that traditional treatment protocols have yet to fully explore or exploit.
From a mechanistic standpoint, cholera patients who recover naturally often stop feeling ill after a day or two but can continue shedding Vibrio cholerae bacteria for up to two weeks. Antibiotic treatment, on the other hand, effectively truncates this infectious phase, quickly halting bacterial shedding even if symptom relief remains relatively constant. Computational models indicate that expanding antibiotic use to moderate cholera cases has the potential to interrupt transmission chains, thereby reducing the number of new infections. This counterintuitive strategy suggests that even though more patients would be using antibiotics, the overall antibiotic consumption across a population during an outbreak could decline due to the decreased disease incidence.
Central to the study’s findings is the delicate balance between individual treatment benefits and population-level epidemiological effects. The researchers constructed a theoretical framework capable of simulating diverse outbreak scenarios by integrating factors such as population density, water sanitation infrastructure, and bacterial transmission rates. Their simulations reveal that in low-to-moderate transmission settings, aggressive antibiotic interventions could substantially curb or even halt outbreaks. In stark contrast, in densely populated regions or those lacking reliable clean water access, the benefits of expanded antibiotic use are insufficient to offset the elevated risk of fostering resistant bacterial strains.
This nuance underscores a critical paradigm shift: antibiotic stewardship in the context of cholera should not solely focus on minimizing use to delay resistance but should also consider strategic usage that suppresses transmission effectively. The model challenges the binary conventional stance of “use antibiotics sparingly” and opens dialogue about context-specific treatment guidelines that consider epidemiological variables alongside individual patient care.
The urgency to rethink cholera management strategies is further amplified by the rising global incidence of the disease. Recent reports have documented a nearly 30% increase in cholera cases and mortality worldwide in just the past year, a spike attributed largely to humanitarian crises such as mass displacement, conflict, and climatic disasters disrupting water and sanitation systems. As climate change intensifies and extreme weather events become more frequent, the vulnerability of previously unaffected regions to cholera outbreaks is expected to grow, making flexible and effective disease control strategies all the more vital.
However, the researchers emphasize that these promising modeling results are preliminary and require validation through more comprehensive simulations and real-world epidemiological studies. Future models need to incorporate additional variables that influence cholera dynamics, such as the deployment of vaccines, variations in population immunity, and healthcare access disparities. Robust “rules of thumb” must be established to help public health officials quickly identify when expanded antibiotic treatment protocols could be implemented safely and effectively.
Furthermore, the study highlights the necessity of sustained surveillance for antibiotic resistance markers in Vibrio cholerae populations following any change in treatment policy. Cholera’s remarkable capacity for developing resistance poses a genuine and immediate threat, making vigilance critical in refining treatment guidelines that balance therapeutic benefits with long-term antibiotic efficacy.
This research offers a data-driven blueprint for reassessing one of the most basic tools in our infectious disease arsenal: antibiotics. As co-first author Dr. Sharia Ahmed notes, “If these findings are further corroborated across diverse settings, we may begin to rethink entrenched policies and harness antibiotics not just for individual recovery but as a public health intervention capable of shaping outbreak trajectories.”
While the authors do not advocate immediate changes to clinical protocols, their findings represent an essential first step towards integrating computational modeling and epidemiological theory into policy-making. Such approaches could profoundly enhance our ability to respond adaptively to cholera outbreaks, especially in an era of evolving global health challenges.
Ultimately, the study encourages a shift from a simplistic “more versus less” antibiotic use debate to a more nuanced discussion encompassing antibiotic timing, population context, and transmission dynamics. This perspective embodies a vital evolution in infectious disease control — one that embraces complexity and leverages advanced modeling to optimize both individual and community health outcomes.
—
Subject of Research: People
Article Title: A theoretical framework to quantify the tradeoff between individual and population benefits of expanded antibiotic use
News Publication Date: 30-Apr-2025
Web References:
https://link.springer.com/article/10.1007/s11538-025-01432-2
https://www.who.int/publications/m/item/multi-country-outbreak-of-cholera–external-situation-report–21—18-december-2024
References:
Keegan, L.T., Ahmed, S.M., et al. A theoretical framework to quantify the tradeoff between individual and population benefits of expanded antibiotic use. Bulletin of Mathematical Biology (2025). DOI: 10.1007/s11538-025-01432-2
Image Credits: Sophia Friesen / University of Utah Health
Keywords: Cholera, Antibiotics, Disease outbreaks, Antibiotic resistance, Epidemiology, Mathematical modeling, Infectious disease transmission
Tags: antibiotic resistance in choleraantibiotic use in cholera treatmentcholera infection and recoverycholera outbreak control strategiescommunity-level cholera transmissionfluid rehydration versus antibiotic treatmentglobal health threats and cholerahealth organization responses to cholerainfectious disease transmission dynamicsinnovative approaches to cholera managementmathematical modeling in public healthreducing cholera infectiousness



{kind=link}