Hydrocephalus is classically seen as a plumbing problem, the result of too much cerebrospinal fluid (CSF) in the brain or dysregulation of fluid flow. It is usually treated with shunts to drain the CSF, or with ETV/CPC, which makes a small hole to drain the CSF and burns off the choroid plexus tissue that produces it. Despite these treatments, some patients have poor neurodevelopmental outcomes.
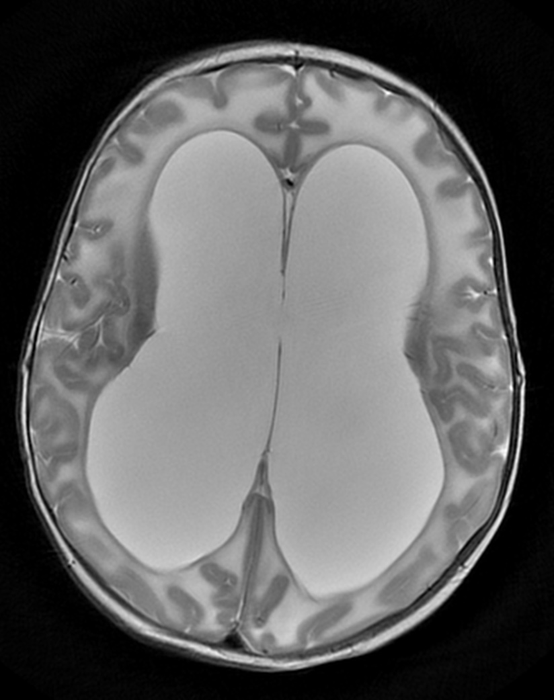
Credit: Phan Q. Duy, PhD
Hydrocephalus is classically seen as a plumbing problem, the result of too much cerebrospinal fluid (CSF) in the brain or dysregulation of fluid flow. It is usually treated with shunts to drain the CSF, or with ETV/CPC, which makes a small hole to drain the CSF and burns off the choroid plexus tissue that produces it. Despite these treatments, some patients have poor neurodevelopmental outcomes.
New research in Nature Neuroscience provides a view of hydrocephalus that turns the “plumbing” concept on its head, at least for some children. It suggests that as many as 1 in 4 congenital cases are genetic, and that the enlarged brain ventricles that characterize hydrocephalus can result not from fluid overaccumulation, but from less brain being formed during fetal development.
“This form of congenital hydrocephalus falls under a radically different paradigm: genetic dysregulation of neural stem cell growth in the brain,” says study leader Kristopher Kahle, MD, PhD, who holds research appointments in Neurosurgery and Genetics and Genomics at Boston Children’s Hospital and is chief of Pediatric Neurosurgery at Massachusetts General Hospital. “When we see enlarged ventricles, the classic thinking is that they reflect too much fluid in the brain. Our study shows that they can reflect brain development that is severely compromised.”
Patients with these genetic mutations may benefit from approaches that optimize neurodevelopment rather than simply draining CSF. The could potentially include targeted drugs, gene editing, or in utero gene therapies could help correct brain development, possibly without neurosurgery.
“Even though we can now treat hydrocephalus endoscopically, without placing a shunt, the consequences of the initial brain injury or developmental anomaly are not reversed,” notes Benjamin Warf, MD, a neurosurgeon in the Hydrocephalus Program at Boston Children’s Hospital. “Understanding more about the various underlying mechanisms of hydrocephalus will lead to therapeutic advances that may not only improve outcomes, but perhaps even prevent hydrocephalus from developing.”
Turning hydrocephalus on its head
Kahle, first author Duy Phan, PhD, an MD/PhD student in the Kahle lab, and other colleagues studied 483 patients with congenital hydrocephalus with whole-exome sequencing. They also sequenced many of the patients’ parents, enabling them identify de novo mutations occurring after conception.
A collection of 93 different genes were associated with hydrocephalus. “We then localized the affected genes’ function in time and space,” says Kahle, who is also an associate member of the Broad Institute.
To do this, the team used single-cell RNA sequencing and consulted atlases of gene transcription in the brain to determine where and at what point in brain development the mutated genes turn on.
The genes’ expression converged in neuroepithelial cells, the earliest-forming neural stem cells. These cells line the embryonic cerebral ventricles in the neural tube during the first several weeks of human brain development, surrounding the developing fluid space.
“This epithelium is critical for populating the rest of the brain with neurons and glia,” says Kahle.
Too few brain cells
The mutations were most commonly in TRIM71, a gene that regulates neural stem cell growth and differentiation. When the team modeled the mutations in mice, the animals developed hydrocephalus, but without showing defects in the flow or reabsorption of CSF.
Further studies revealed that the stem cells in the neuroepithelium differentiated too soon in embryonic development. Cell proliferation was decreased, with fewer neurons than would be expected. This led to an underdeveloped cortex.
“Perhaps most notably, this underdevelopment results in a ‘floppy’ cortex that is unable to hold the pressure exerted by fluid in the ventricles,” says Phan. “Thus, fluid passively accumulates and distends the ventricles even when there is no anatomical obstruction to CSF flow.”
A clinical agenda
Kahle and Phan now plan to continue genetic sequencing of patients with hydrocephalus and correlate the results with clinical findings, in collaboration with Christopher Walsh, MD, PhD, chief of Genetics and Genomics at Boston Children’s and an expert in neurodevelopmental genetics. They will also compare genetic results with fetal and infant neuroimaging studies to establish a diagnostic MRI “signature” for genetic hydrocephalus.
“This work suggests that genetic testing should be considered for a larger slice of patients with hydrocephalus that we might have previously suspected,” says Walsh. “Experience always shows that the more we learn about underlying mechanisms, the closer we come to individualizing treatment approaches.”
In collaboration with Boston Children’s neurosurgeons, including Warf, Scellig Stone, MD, PhD, and Mark Proctor, MD, Kahle also plans to correlate genetic profiles with patients’ outcomes after receiving shunts or ETV/CPC.
“There are scattered reports of kids not improving after being shunted, and ventricular size not changing,” Kahle says. “Some patients may benefit from more conservative management.”
This work was supported by the National Institutes of Health (T32GM136651, F30HD106694, RO1NS11102, 1R21NS121642-01, 1R01NS122904-01, 5R21NS116484-02, 1DP2AI138259-01, MH113257, DA023999), the David M. Rubenstein Fund for Hearing Research, the Rudi Schulte Institute, the Hydrocephalus Association, the National Heart, Lung, and Blood Institute (R00HL143036-02), the Clinical & Translational Research Funding Program (CTSA1405), Children’s Discovery Institute (CDI-FR-2021-926), the Burroughs Welcome Fund, the Hartwell Foundation, and Deutsche Forschungsgemeinschaft (German Research Foundation) (WU 563/3-1, EXC2151–390873048).
About Boston Children’s Hospital
Boston Children’s Hospital is ranked the #1 children’s hospital in the nation by U.S. News & World Report and is the primary pediatric teaching affiliate of Harvard Medical School. Home to the world’s largest research enterprise based at a pediatric medical center, its discoveries have benefited both children and adults since 1869. Today, 3,000 researchers and scientific staff, including 11 members of the National Academy of Sciences, 25 members of the National Academy of Medicine and 10 Howard Hughes Medical Investigators comprise Boston Children’s research community. Founded as a 20-bed hospital for children, Boston Children’s is now a 415-bed comprehensive center for pediatric and adolescent health care. For more, visit our Answers blog and follow us on social media @BostonChildrens, @BCH_Innovation, Facebook and YouTube.
– ### –
Journal
Nature Neuroscience
DOI
10.1038/s41593-022-01043-3
COI Statement
Coauthor Jane Juusola is an employee of GeneDx, Inc.


{kind=link}