(New York, NY – December 12, 2016) — Even before tumors develop, breast cancer cells with a few defined molecular alterations can spread to organs, remain quiet for long periods of time, and then awaken to form aggressive, deadly breast cancer metastasis, says a team of investigators led by researchers at Icahn School of Medicine at Mount Sinai and the University of Regensburg in Germany.
They say their finding, published in two papers in the journal Nature, and conducted in animal models and tested in human samples, now solves the mystery of how breast cancer metastasis forms without a primary tumor in this new model of early dissemination and metastasis. Furthermore, a clinical primary tumor may never develop, investigators say.
The University of Regensburg team had discovered that cancer cells could spread not only from a highly mutated, overtly evolved and pathologically-defined invasive tumors, but also from early stage cancers commonly considered incapable of spreading cells. However, how these early cancer lesions could spawn cells with traits of malignant tumors was unknown.
In two papers published in the journal Nature, and conducted in animal models and tested in human samples, the two teams now have identified the first mechanisms that allow cells to spread early in cancer progression and contribute to metastasis.
In the study from Mount Sinai, two changes in mammary cancer cells — a switched-on oncogene and a turned-off tumor suppressor– motivated cells to travel from breast tissue to the lungs and other parts of the body. There, the cells stayed quiet until a growth switch was activated and metastases developed in lungs.
"This research provides insight into the mechanisms of early cancer spread and may shed light into unexplained phenomena — among them, why as many as 5 percent of cancer patients worldwide have cancer metastases but no original tumor, and most importantly, why it is so difficult to treat cancer that has spread," says the study's senior investigators, Julio A. Aguirre-Ghiso, PhD, Professor of Medicine, Hematology and Medical Oncology, Maria Soledad Sosa, PhD, Assistant Professor of Pharmacological Sciences, and graduate student Kathryn Harper of The Tisch Cancer Institute at the Icahn School of Medicine at Mount Sinai.
"Biologically, this new model of early metastasis challenges everything we thought we knew about how cancer spreads and forms metastasis. It feels like we are going to have to adjust our ideas about the subject of metastasis," he says. "Our hope is that these findings will reshape the way we think about how metastasis should be treated."
An important finding from the Mount Sinai team is that most early spread cells remain dormant and most chemotherapy and targeted therapies are aimed at those cells that are proliferative. So early spread cancer cells would escape these conventional therapies even if it kills a primary tumor, Dr. Aguirre-Ghiso says. The work also poses new questions on how early spread cancer cells support metastasis development. Do they do it on their own, do they set the soil for later arriving cells from tumors not caught early, or do they cooperate with later arriving cells? This study reveals a new biological mechanism of early dissemination that must be explored to fully understand how to target the seeds of metastasis.
The companion paper headed by Dr. Christoph Klein at the University of Regensburg in Germany, published in the same issue of Nature and co-authored by Dr. Aguirre-Ghiso and members of his team provides additional key mechanistic clues on how early spread is controlled and proof in human cancer cells and tumors of the preclinical findings in this study. Researchers from both teams arrived at their findings independently and then collaborated on the project.
Researchers from both teams studied very early stages of breast cancer including DCIS (ductal carcinoma in situ), a noninvasive breast lesion, since 2-3 percent of women who have been treated for DCIS die of metastasis without ever developing a primary tumor. "The best explanation for this phenomenon is that early metastasis occurs before or as DCIS develops. A key finding from this second paper is that in the mouse models, 80% of metastasis originated from the early spread cells and not from the large tumors. In fact, the Klein group identified a mechanism by which spread is more efficient in early lesions than in large tumors.
In both studies, investigators found that early cancer cell spread is an extension of the normal process of creating a branching tree of breast milk ducts in females.
Two major pathways are activated in this ancient process — p38, a tumor suppressor, and HER2, an oncogene. Switching off p38 and turning on HER2 activates a module of the EMT (epithelial to mesenchymal transition) signaling pathway. EMT promotes movement of cells during embryogenesis and tissue development. The Klein paper also shows that progesterone receptor signaling, which controls branching of the mammary tree, is important for this early spread by regulating cues involved in EMT and growth programs, a mechanism that was hinted in his earlier studies.
As a mammary tree develops, p38, HER2, and EMT are alternatively turned on and off. This, in cooperation with progesterone signaling, allows mammary cells to move through the mammary gland, hollow out a tubular, branching network of milk ducts that flow to the nipple.
"Tweaking these pathways are a normal way of forming hollow branching tubes," Dr. Aguirre-Ghiso says. But in their experiments, they found that if HER2 is over-activated (not switched off) or mutated, and p38 is permanently turned off, EMT was continually activated, allowing cells to move out of the mammary gland and into the animal's body through the blood.
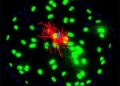
"We were able to use organoids in three-dimensional cultures, and high resolution imaging directly in the live animal models to actually see these cells enter the blood stream from the mammary tree and travel to the lung, the bone marrow, and other places," he says. "We hadn't thought about oncogenes and tumor suppressors in this way before. This is a new function for these pathways."
John S. Condeelis, PhD, co-Director of the Gruss Lipper Biophotonics Center and its Integrated Imaging Program at Einstein, where the high resolution intravital imaging was performed, noted that "We were surprised to learn that cancer cells from DCIS-like lesions could show such robust dissemination using similar machinery found in tumor cells from invasive carcinoma. This is a new insight with implications beyond our expectations." Also David Entenberg MSc, Director of Technological Development and Intravital Imaging who led the imaging efforts within the same Center said, "A few years ago, it would not have been possible to image these disseminating cells inside a living animal with this level of detail. We're pleased that Einstein's imaging technology could, through this collaboration, contribute to the definitive proof of early dissemination."
And while both studies focus on the mechanisms of early dissemination in breast cancer, similar processes could control early dissemination and metastasis in other human cancers, including melanoma and pancreatic cancer. In fact, pancreatic cancer early dissemination has also been linked to an EMT process, Dr. Aguirre-Ghiso says.
Among the critical avenues they are investigating, Mount Sinai researchers are looking for the growth switch that pushes early spread of dormant cancer cells to form metastases. "While our findings add a whole new level of complexity to the understanding of cancer, they also add energy to our efforts to finally solve the big issue in cancer — stop the metastasis that kills patients," Dr. Aguirre-Ghiso says.
###
Study contributors include lead co-authors Kathryn L. Harper, PhD, Maria Soledad Sosa, PhD, Julie F. Cheung, BSc, Rita Nobre MSc, Alvaro Avivar-Valderas, PhD, Chandandaneep Nagi, MD, and Eduardo F. Farias, PhD, from Icahn School of Medicine at Mount Sinai; Christoph Klein, MD and Hedayatollah Hosseini, PhD from the University of Regensburg, Germany; Nomeda Girnius, PhD and Roger J. Davis, PhD from Howard Hughes Medical Institute at the University of Massachusetts Medical School; and David Entenberg, MSc and John Condeelis, PhD from Albert Einstein College of Medicine in New York.
The study was supported by grants SWCRF, CA109182, CA196521, CA163131, CA100324, F31CA183185, BC132674, BC112380, NIH 1S10RR024745 Microscopy CoRE at ISMMS, the Integrated Imaging Program at Einstein, HHMI, DFG KL 1233/10-1 and the ERC (322602).
For a video on this release: https://youtu.be/MvPpghwr4Is
About the Mount Sinai Health System
The Mount Sinai Health System is an integrated health system committed to providing distinguished care, conducting transformative research, and advancing biomedical education. Structured around seven hospital campuses and a single medical school, the Health System has an extensive ambulatory network and a range of inpatient and outpatient services–from community-based facilities to tertiary and quaternary care.
The System includes approximately 7,100 primary and specialty care physicians; 12 joint-venture ambulatory surgery centers; more than 140 ambulatory practices throughout the five boroughs of New York City, Westchester, Long Island, and Florida; and 31 affiliated community health centers. Physicians are affiliated with the renowned Icahn School of Medicine at Mount Sinai, which is ranked among the highest in the nation in National Institutes of Health funding per investigator. The Mount Sinai Hospital is on the "Honor Roll" of best hospitals in America, ranked No. 15 nationally in the 2016-2017 "Best Hospitals" issue of U.S. News & World Report. The Mount Sinai Hospital is also ranked as one of the nation's top 20 hospitals in Geriatrics, Gastroenterology/GI Surgery, Cardiology/Heart Surgery, Diabetes/Endocrinology, Nephrology, Neurology/Neurosurgery, and Ear, Nose & Throat, and is in the top 50 in four other specialties. New York Eye and Ear Infirmary of Mount Sinai is ranked No. 10 nationally for Ophthalmology, while Mount Sinai Beth Israel, Mount Sinai St. Luke's, and Mount Sinai West are ranked regionally. Mount Sinai's Kravis Children's Hospital is ranked in seven out of ten pediatric specialties by U.S. News & World Report in "Best Children's Hospitals."
For more information, visit http://www.mountsinai.org or find Mount Sinai on Facebook, Twitter and YouTube.
Media Contact
Marlene Naanes
[email protected]
646-605-7687
@mountsinainyc
http://www.mountsinai.org
############
Story Source: Materials provided by Scienmag