Your nose is not the only organ in your body that can sense cigarette smoke wafting through the air. Scientists at Washington University in St. Louis and the University of Iowa have shown that your lungs have odor receptors as well.
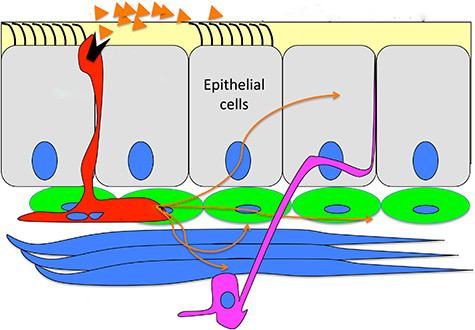
Unlike the receptors in your nose, which are located in the membranes of nerve cells, the ones in your lungs are in the membranes of neuroendocrine cells. Instead of sending nerve impulses to your brain that allow it to “perceive” the acrid smell of a burning cigarette somewhere in the vicinity, they trigger the flask-shaped neuroendocrine cells to dump hormones that make your airways constrict.
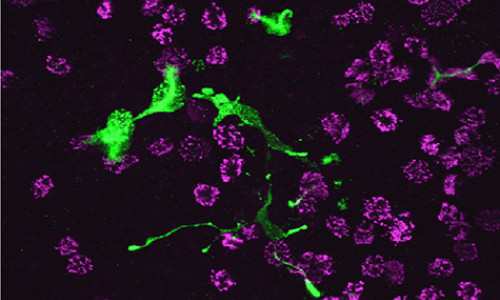
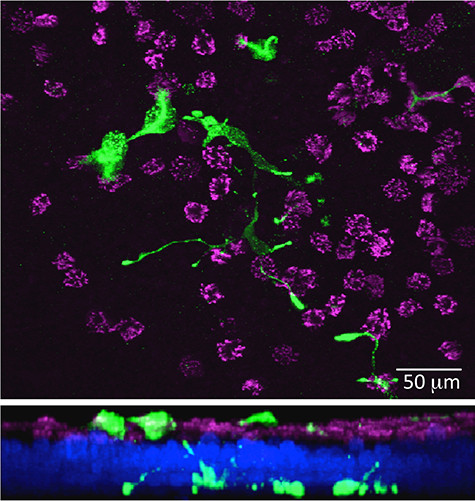
The newly discovered class of cells expressing olfactory receptors in human airways, called pulmonary neuroendocrine cells, or PNECs, were found by a team led by Yehuda Ben-Shahar, PhD, assistant professor of biology, in Arts & Sciences, and of medicine at Washington University in St. Louis, and including colleagues Steven L. Brody, MD, and Michael J. Holtzman, MD, of the Washington University School of Medicine, and Michel J. Welsh, MD, of the University of Iowa Carver College of Medicine.
“We forget,” said Ben-Shahar, “that our body plan is a tube within a tube, so our lungs and our gut are open to the external environment. Although they’re inside us, they’re actually part of our external layer. So they constantly suffer environmental insults,” he said, “and it makes sense that we evolved mechanisms to protect ourselves.”
In other words, the PNECs, described in the March issue of the American Journal of Respiratory Cell and Molecular Biology, are sentinels, guards whose job it is to exclude irritating or toxic chemicals.
The cells might be responsible for the chemical hypersensitivity that characterizes respiratory diseases, such as chronic obstructive pulmonary disease (COPD) and asthma. Patients with these diseases are told to avoid traffic fumes, pungent odors, perfumes and similar irritants, which can trigger airway constriction and breathing difficulties.
The odor receptors on the cells might be a therapeutic target, Ben-Shahar suggests. By blocking them, it might be possible to prevent some attacks, allowing people to cut down on the use of steroids or bronchodilators.
Every breath you take
When a mammal inhales, volatile chemicals flow over two patches of specialized epithelial tissue high up in the nasal passages. These patches are rich in nerve cells with specialized odorant-binding molecules embedded in their membranes.
If a chemical docks on one of these receptors, the neuron fires, sending impulses along the olfactory nerve to the olfactory bulb in the brain, where the signal is integrated with those from hundreds of other similar cells to conjure the scent of old leather or dried lavender.
Aware that airway diseases are characterized by hypersensitivity to volatile stimuli, Ben-Shahar and his colleagues realized that the lungs, like the nose, must have some means of detecting inhaled chemicals.
Earlier, a team at the University of Iowa, where Ben-Shahar was a postdoctoral research associate, had searched for genes expressed by patches of tissue from lung transplant donors. They found a group of ciliated cells that express bitter taste receptors. When offending substances were detected, the cilia beat more strongly to sweep them out of the airway. This result was featured on the cover of the Aug. 28, 2009, issue of Science.
But since people are sensitive to many inhaled substances, not just bitter ones, Ben-Shahar decided to look again. This time he found that these tissues also express odor receptors, not on ciliated cells but instead on neuroendocrine cells, flask-shaped cells that dump serotonin and various neuropeptides when they are stimulated.
This made sense. “When people with airway disease have pathological responses to odors, they’re usually pretty fast and violent,” said Ben-Shahar. “Patients suddenly shut down and can’t breathe, and these cells may explain why.”
Ben-Shahar stresses the differences between chemosensation in the nose and in the lung. The cells in the nose are neurons, he points out, each with a narrowly tuned receptor, and their signals must be woven together in the brain to interpret our odor environment.
The cells in the airways are secretory, not neuronal, cells, and they may carry more than one receptor, so they are broadly tuned. Instead of sending nerve impulses to the brain, they flood local nerves and muscles with serotonin and neuropeptides. “They are possibly designed,” he said, “to elicit a rapid, physiological response if you inhale something that is bad for you.”
The different mechanisms explain why cognition plays a much stronger role in taste and smell than in coughing in response to an irritant. It is possible, for example, to develop a taste for beer. But nobody learns not to cough; the response is rapid and largely automatic.
The scientists suspect these pulmonary neuroscretory cells contribute to the hypersensitivity of patients with COPD to airborne irritants. COPD is a group of diseases, including emphysema, that is characterized by coughing, wheezing, shortness of breath and chest tightness.
When the scientists looked at the airway tissues from patients with COPD, they discovered that they had more of these neurosecretory cells than airway tissues from healthy donors.
Of mice and men
As a geneticist, Ben-Shahar would like to go farther, knocking out genes to make sure that the derangement of neurosecretory cells isn’t just correlated with airway diseases but instead suffices to produce it.
But there is a problem. “For example, a liver from a mouse and a liver from a human are pretty similar, they express the same types of cells. But the lungs from different mammalian species are often very different; you can see it at a glance,” Ben-Shahar said.
“Clearly, primates have evolved distinct cell lineages and signaling systems for respiratory-specific functions.”
This makes it challenging to unravel the biomolecular mechanisms of respiratory diseases.
Still, he is hopeful that the PNEC pathways will provide targets for drugs that would better control asthma, COPD and other respiratory diseases. They would be welcome. There has been a steep rise in these diseases in the past few decades, treatment options have been limited, and there are no cures.
Story Source:
The above story is based on materials provided by Washington University in St. Louis, Diana Lutz.
Image credits: BEN-SHAHAR



{kind=link}