Treating cancer with immunotherapies known as an immune checkpoint blockade (ICB) prior to surgery (so-called neoadjuvant immunotherapy) has been a rapidly growing area of research, but the scientific community is just scratching the surface of what is possible, according to a review article co-authored by several current and former investigators from the Bloomberg~Kimmel Institute for Cancer Immunotherapy and the Johns Hopkins Kimmel Cancer Center.
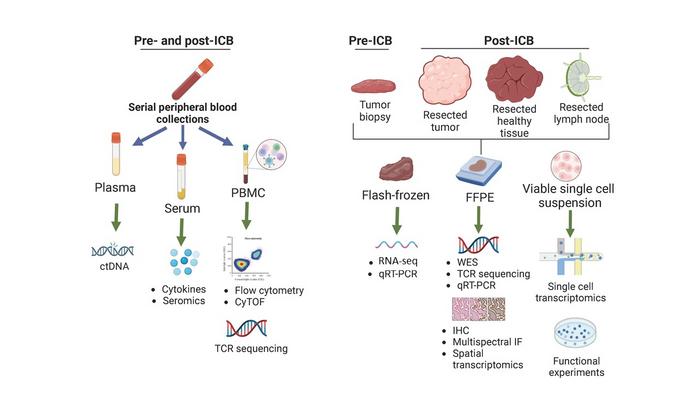
Credit: Graphic courtesy of Cancer Cell
Treating cancer with immunotherapies known as an immune checkpoint blockade (ICB) prior to surgery (so-called neoadjuvant immunotherapy) has been a rapidly growing area of research, but the scientific community is just scratching the surface of what is possible, according to a review article co-authored by several current and former investigators from the Bloomberg~Kimmel Institute for Cancer Immunotherapy and the Johns Hopkins Kimmel Cancer Center.
“We consider this approach to cancer immunotherapy to be a gold mine for advancing our scientific knowledge of how an immune checkpoint blockade is working, to define better biomarkers that predict clinical outcomes, and to help us design the next generation of more effective treatments with combination therapies,” says lead author Suzanne Topalian, M.D., director of the Johns Hopkins Melanoma/Skin Cancer Program and associate director of the Bloomberg~Kimmel Institute for Cancer Immunotherapy.
Neoadjuvant ICB is being tested across multiple types of cancer in hundreds of clinical trials. Some neoadjuvant ICB regimens in certain tumors have led to pathologic complete responses, meaning no microscopic evidence of residual live tumor cells in the surgical specimen. The review paper, published Sept. 11 in the journal Cancer Cell, highlights notable clinical studies using ICB in lung cancer, triple-negative breast cancer, melanoma and non-melanoma skin cancers, and gastrointestinal cancers that have established cross-cutting principles for this treatment approach. Neoadjuvant ICB is still largely experimental, but there have been recent FDA approvals in triple-negative breast cancer and lung cancer, and more approvals are anticipated.
In lung cancers, the reviewers note, changes that happen in cancer tissue after ICB occur much more rapidly than what can be seen on CT scans in standard oncology practice. In some cases, a mass that may still be visible on CT scanning contains no live tumor cells when experts go to operate and look under a microscope. In the setting of neoadjuvant ICB, pathologic response can tell researchers more about treatment effects than radiographic response, Topalian says.
From ICB trials in triple-negative breast cancer, investigators have learned that a combination of chemotherapy plus ICB can be effective in preventing post-surgical relapse, and that giving ICB to patients with earlier-stage cancers prior to surgery is more effective than giving it to patients with advanced, inoperable disease. In skin cancers, investigators have learned that combination therapies can be helpful but not always needed, and that some patients who have complete responses as seen under a microscope may not need extensive medical treatment. In gastrointestinal cancers, investigators have learned that a genetically defined group of GI cancers called MSI-high responds so well to neoadjuvant ICB that some patients may not even need surgery.
A number of themes are emerging from ICB clinical trials, the authors say:
- Immunotherapy regimens that show significant efficacy against advanced, inoperable cancers also tend to be effective when given prior to surgery.
- The degree of pathologic response after neoadjuvant ICB predicts the relapse-free time interval after surgery.
- Neoadjuvant ICB may not only prime anti-tumor activity in the immune system, but can also have a positive effect on surgery, either shrinking tumors to the point where removing them is less disfiguring or potentially making surgery unnecessary.
- Surgically removed tissues after neoadjuvant ICB offer a unique resource for in-depth scientific studies to learn more about how ICB works, and about how to overcome treatment resistance.
Topalian and co-lead author Drew Pardoll, M.D., Ph.D., director of the Bloomberg~Kimmel Institute for Cancer Immunotherapy, are available for comment. Other authors who contributed to this review were Leisha Emens, M.D., Ph.D., formerly of Johns Hopkins; Patrick Forde, M.B.B.Ch.; Kellie Smith, Ph.D.; and Mark Yarchoan, M.D.
Journal
Cancer Cell

