Hepatocellular carcinoma (HCC) is one of the most prevalent malignancies globally and is the third leading cause of cancer-related deaths. The primary curative treatments for HCC are liver transplantation, hepatectomy, and local ablation. However, the recurrence rate of HCC following hepatectomy or ablation remains alarmingly high, up to 70%, severely impacting patient prognosis and overall survival (OS). To mitigate postoperative recurrence and improve patient outcomes, various adjuvant therapies have been explored. Despite the efficacy of several adjuvant treatments in reducing recurrence rates and enhancing survival, there is no standardized consensus on their application across national guidelines, leading to significant disparities in recommendations between Eastern and Western medical practices.
Credit: Jian-Hong Zhong, Liang Ma, Le Li, Zhen-Zhen Li
Hepatocellular carcinoma (HCC) is one of the most prevalent malignancies globally and is the third leading cause of cancer-related deaths. The primary curative treatments for HCC are liver transplantation, hepatectomy, and local ablation. However, the recurrence rate of HCC following hepatectomy or ablation remains alarmingly high, up to 70%, severely impacting patient prognosis and overall survival (OS). To mitigate postoperative recurrence and improve patient outcomes, various adjuvant therapies have been explored. Despite the efficacy of several adjuvant treatments in reducing recurrence rates and enhancing survival, there is no standardized consensus on their application across national guidelines, leading to significant disparities in recommendations between Eastern and Western medical practices.
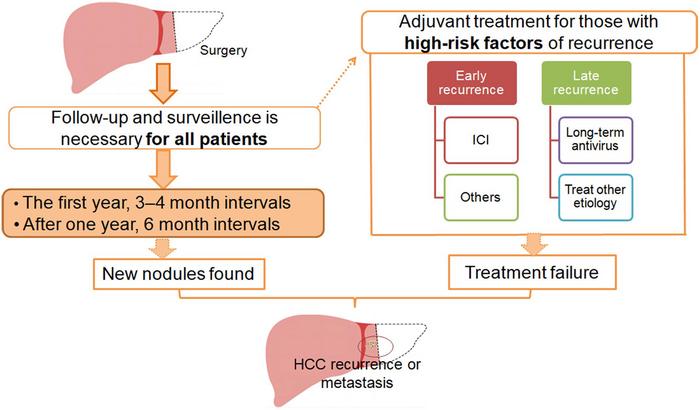
HCC recurrence can generally be classified into two categories: early recurrence, which typically occurs within two years post-treatment, and late recurrence, which occurs after two years. Early recurrence is often linked to intrahepatic micrometastases or microthrombi from the primary tumor, whereas late recurrence is usually associated with multicentric new tumor formations. Risk factors for early recurrence include large tumor size (>5 cm), multiple tumors, the presence of satellite lesions, lack of a tumor capsule, tumor rupture, non-anatomical resection, narrow resection margins (≤2 cm), high alpha-fetoprotein levels (≥400 ng/mL), and microvascular or macrovascular invasion. Conversely, late-recurrence risk factors include liver cirrhosis, higher hepatitis activity grades, and poor tumor classification.
The primary aim of adjuvant therapy following local treatments like hepatectomy or ablation is to reduce the recurrence rate and thus improve recurrence-free survival (RFS) and OS. The choice of adjuvant therapy should be guided by the risk factors specific to early or late recurrence.
- Antiviral Therapy: For patients with hepatitis-related HCC, antiviral therapy aims to inhibit long-term viral replication, reduce liver damage, prevent disease progression, and ultimately prolong survival. For HCV-related HCC, sustained viral eradication using interferon-based or interferon-free regimens significantly reduces recurrence. Similarly, for HBV-related HCC, nucleos(t)ide analogs such as tenofovir and entecavir are recommended. Studies have shown that tenofovir is particularly effective in reducing recurrence and improving survival compared to entecavir.
- Transarterial Chemoembolization (TACE): This is often used as an adjuvant therapy for patients at high risk of intrahepatic metastasis. TACE targets disseminated tumor cells that have spread from the primary tumor, helping to reduce early recurrence by effectively eliminating residual tumors.
- Immune Checkpoint Inhibitors (ICIs): Recent guidelines, particularly in the United States, have begun to include recommendations for ICIs in the adjuvant setting. ICIs help boost the body’s antitumor immunity and have shown promise in reducing recurrence rates and improving survival outcomes in HCC patients.
Despite the promising results of various adjuvant therapies, there remain several unanswered questions and challenges. The lack of a universally accepted standard for adjuvant therapy in HCC highlights the need for further research and clinical trials to establish clear guidelines. Moreover, the balance between the benefits and potential adverse effects of adjuvant treatments must be carefully considered to optimize patient outcomes. Future studies should aim to refine patient selection criteria for adjuvant therapies, tailoring treatments based on individual risk profiles to maximize efficacy and minimize harm.
In conclusion, while significant strides have been made in the development of adjuvant therapies for HCC, ongoing research and international collaboration are essential to standardize treatment protocols and improve the prognosis for HCC patients worldwide.
Full text
https://www.xiahepublishing.com/2310-8819/JCTH-2024-00030
The study was recently published in the Journal of Clinical and Translational Hepatology.
The Journal of Clinical and Translational Hepatology (JCTH) is owned by the Second Affiliated Hospital of Chongqing Medical University and published by XIA & HE Publishing Inc. JCTH publishes high quality, peer reviewed studies in the translational and clinical human health sciences of liver diseases. JCTH has established high standards for publication of original research, which are characterized by a study’s novelty, quality, and ethical conduct in the scientific process as well as in the communication of the research findings. Each issue includes articles by leading authorities on topics in hepatology that are germane to the most current challenges in the field. Special features include reports on the latest advances in drug development and technology that are relevant to liver diseases. Regular features of JCTH also include editorials, correspondences and invited commentaries on rapidly progressing areas in hepatology. All articles published by JCTH, both solicited and unsolicited, must pass our rigorous peer review process.
Follow us on X: @xiahepublishing
Follow us on LinkedIn: Xia & He Publishing Inc.
Journal
Journal of Clinical and Translational Hepatology
DOI
10.14218/JCTH.2024.00030
Article Title
Adjuvant Therapy for Hepatocellular Carcinoma After Curative Treatment: Several Unanswered Questions
Article Publication Date
24-Apr-2024

