In a groundbreaking exploration of neonatal care technology, a recent national multidisciplinary survey has unveiled critical insights into the availability, utilization, and barriers surrounding the use of bowel ultrasound (BUS) for diagnosing and managing necrotizing enterocolitis (NEC). NEC, a devastating gastrointestinal disease primarily afflicting premature infants, remains a challenge for neonatologists due to its rapid progression and high mortality rates. The survey highlights the expanding role of BUS as a frontline diagnostic tool, offering a radiation-free, real-time imaging method that holds promise for revolutionizing neonatal intensive care units (NICUs).
Over the past decade, bowel ultrasound has emerged as a pivotal diagnostic adjunct in identifying NEC earlier than traditional radiographic methods. However, its widespread adoption has been inconsistent, prompting researchers to probe the systemic issues influencing access and implementation. The study systematically gathered feedback from neonatologists, pediatric surgeons, and radiologists across a diverse array of institutions, mapping the intricate landscape of BUS integration within clinical protocols.
The findings reveal a nuanced disparity in BUS availability that correlates strongly with institutional resources and geographic location. High-tier academic centers tend to have dedicated radiology support, enabling regular access to BUS, while smaller or community hospitals frequently encounter logistical hindrances. These disparities extend to workload allocations, where trained sonographers and specialized clinicians proficient in BUS interpretation are notably limited, impeding timely imaging and clinical decision-making.
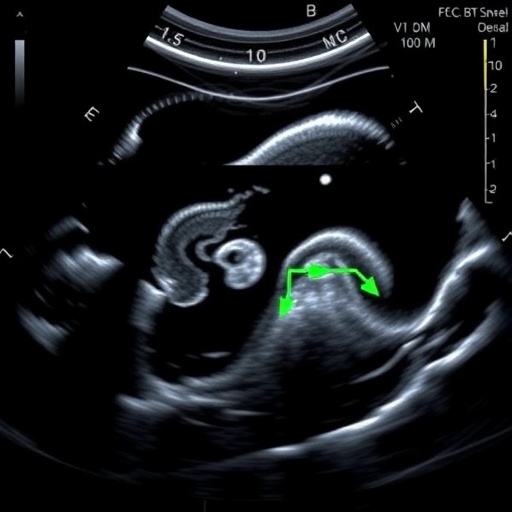
Utilization rates of bowel ultrasound further elucidate the divide between potential and practice. Where available, BUS is employed selectively rather than as a routine monitoring tool for at-risk neonates. This conservative approach appears tied to both entrenched reliance on abdominal radiographs and skepticism regarding the sensitivity and specificity of ultrasound findings in NEC. Nonetheless, emerging evidence underscores BUS’s superiority in detecting bowel wall thickening, pneumatosis intestinalis, and portal venous gas—hallmarks of NEC that are often subtle or delayed on X-rays.
Interprofessional collaboration surfaces as a crucial determinant in BUS deployment. The survey indicates that when neonatologists and radiologists engage in ongoing dialogue and joint training sessions, confidence in BUS utilization markedly increases. Conversely, lack of standardized protocols and variability in ultrasound technique contribute to interpretative uncertainties, fostering resistance to adopting BUS as a standard of care. The absence of nationally endorsed guidelines for BUS in NEC underscores a pressing need for consensus-building within the pediatric community.
Intriguingly, the technological sophistication of ultrasound equipment also plays a role in effective usage. Institutions with access to high-resolution probes and portable units report smoother incorporation of BUS into bedside assessments. Portable ultrasound devices are particularly advantageous in NICUs, allowing real-time imaging at the incubator without transferring critically ill infants, thereby reducing infection risk and transport-associated stress.
The study delves into educational deficits as a barrier, revealing that many clinicians feel underprepared to perform or interpret bowel ultrasounds confidently. Minimal inclusion of BUS training in neonatology fellowships and radiology residencies leaves a knowledge gap that hinders proficiency. Addressing this requires integrating focused curricula and simulation-based training dedicated to neonatal bowel pathology and sonographic patterns indicative of NEC.
Financial constraints also emerge as a palpable obstacle, especially in underfunded centers where investment in ultrasound machines and dedicated personnel is prohibitive. While BUS could potentially curtail costs by decreasing reliance on radiographs and improving early diagnosis, initial outlay and ongoing maintenance expenses limit implementation in resource-limited settings. Stakeholders highlight the need for demonstrating cost-effectiveness to convince hospital administrators and healthcare policymakers.
The clinical implications of enhancing BUS accessibility are profound. Early and accurate detection of NEC can dramatically alter patient trajectories, enabling prompt surgical consultations or targeted medical therapy. Furthermore, BUS can assist in monitoring disease progression, guiding nutritional management, and alerting clinicians to complications like bowel perforation or strictures, which demand immediate intervention.
The research advocates for forging robust multidisciplinary partnerships to overcome existing hurdles. Such collaboration could pave the way for standardized training modules, user-friendly imaging protocols, and quality assurance measures designed to elevate BUS reliability. By fostering interdisciplinary trust and knowledge sharing, the neonatal care community can better harness the full potential of bowel ultrasound in combating NEC.
Moreover, the integration of advanced imaging technologies such as contrast-enhanced ultrasound and elastography is yet to be explored fully in this context but offers exciting avenues for future exploration. These modalities could enrich diagnostic accuracy, providing functional insights into bowel perfusion and tissue integrity, potentially improving NEC outcomes further.
In reflecting on this comprehensive survey, the urgency for concerted action becomes evident. Addressing the layered barriers—from logistical, technological, educational, and financial perspectives—requires strategic planning at institutional and national levels. Incentivizing BUS adoption through research funding, quality improvement initiatives, and policy reforms could bridge existing gaps.
Ultimately, this study calls the neonatal care field to recognize bowel ultrasound not just as an ancillary tool, but as a transformative modality with the capacity to reshape the diagnostic paradigm for NEC. Empowering clinicians with access, skills, and confidence in BUS may set new standards in neonatal gastrointestinal imaging, promising a future where early, precise, and non-invasive diagnosis saves countless infant lives.
As the community responds to these findings, the next wave of innovations will likely focus on enhancing ultrasound image interpretation through artificial intelligence and machine learning. Integrating these technologies could support less experienced practitioners, standardize assessments, and contribute to more objective clinical decision-making.
The implications extend beyond NEC alone. BUS’s utility could broaden to encompass a spectrum of neonatal bowel disorders, post-operative monitoring, and even guiding minimally invasive interventions. Establishing a foundation now ensures that neonatal care evolves in concert with technological advances, ultimately optimizing outcomes for the most vulnerable patients.
This landmark survey provides a compelling roadmap for improving neonatal gastrointestinal imaging infrastructure and clinical practice. The challenge ahead lies in translating these insights into actionable change that elevates bowel ultrasound from promising concept to indispensable clinical mainstay in the battle against necrotizing enterocolitis.
Subject of Research: Availability, utilization, and barriers to bowel ultrasound (BUS) for necrotizing enterocolitis (NEC)
Article Title: Availability, utilization, and barriers to bowel ultrasound for necrotizing enterocolitis: a national multidisciplinary survey
Article References:
Cuna, A., Thai, J.D., McNelis, K. et al. Availability, utilization, and barriers to bowel ultrasound for necrotizing enterocolitis: a national multidisciplinary survey. J Perinatol (2026). https://doi.org/10.1038/s41372-026-02677-y
Image Credits: AI Generated
DOI: 09 April 2026
Tags: access to bowel ultrasound in NICUsbowel ultrasound for necrotizing enterocolitischallenges in NEC imagingdisparities in neonatal imaging resourcesgeographic variation in NEC diagnostic toolsimpact of institutional resources on NEC diagnosisimplementation barriers for bowel ultrasoundmultidisciplinary survey on neonatal careNEC diagnosis in premature infantsneonatal bowel ultrasound diagnosticsrole of radiologists in neonatal NEC careultrasound vs radiography for NEC


{kind=link}