Credit: Copyright © 2021, Jun Nakayama, Shinshu University
Helicobacter pylori (H. pylori), a gram-negative pathogen that has infected half of the world’s population is a Group I carcinogen according to the WHO. H. pylori resides in the gastric mucosa causing gastritis, ulcers, gastric cancers and malignant lymphoma of the stomach. It can be eradicated in most infected people using a combination of three drugs; antibiotics clarithromycin, amoxicillin, and gastric acid suppressants. Amoxicillin exerts antibacterial activity by inhibiting the biosynthesis of peptidoglycan present in the cell wall of bacteria, and clarithromycin exerts antibacterial activity by inhibiting protein synthesis.
The current success rate of H. pylori eradication is about 90%. Metronidazole is used instead of clarithromycin for secondary eradication, but the eradication success rate is still 75%, and drug-resistant H. pylori is a growing problem. Therefore, it is expected to develop drugs that exhibit anti-H. pylori activity by a mechanism different from those of these antibiotics.
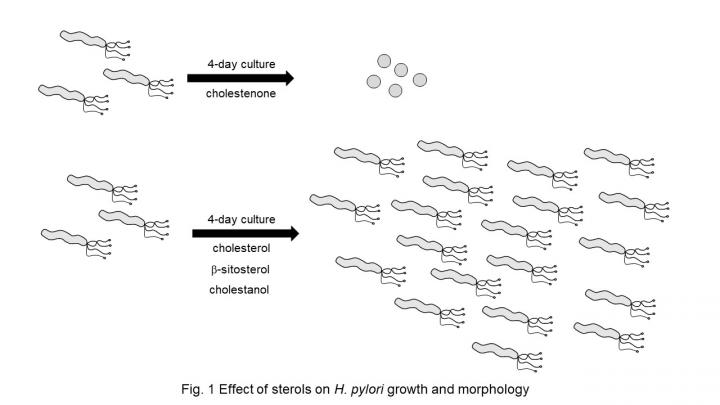
Cholestenone is a cholesterol analog catabolized by intestinal bacteria. In a study led by Dr. Jun Nakayama of the Department of Molecular Pathology, Shinshu University School of Medicine, cholestenone was found to inhibit biosynthesis of the cell wall of the H. pylori, suppressing its growth. The cell wall of H. pylori contains a molecule called cholesteryl α-D-glucopyranoside (CGL). CGL is important for the survival of H. pylori and is biosynthesized from cholesterol around H. pylori. This study showed that the growth of H. pylori was inhibited and its morphology changed from spiral to spherical after 4 days of incubation in the presence of cholestenone. On the other hand, when H. pylori was cultured for 4 days in the presence of cholesterol, β-sitosterol, and cholestanol as sterols with a hydroxyl group at the 3-position, neither growth inhibition nor abnormal morphology of the bacteria was observed (Fig. 1). In addition, CGL biosynthesis was suppressed in H. pylori cultured in the presence of cholestenone, indicating that cholestenone exhibits antibacterial activity by inhibiting CGL biosynthesis. H. pylori growth suppression by cholestenone was also effective against a clinically isolated clarithromycin-resistant H. pylori strain. Furthermore, mice fed a cholestenone-containing diet showed significant eradication of H. pylori in the gastric mucosa. This suggests that cholestenone could be used as an oral medicine to treat H. pylori patients.
Professor Nakayama’s research group previously showed that α1,4-linked N-acetylglucosamine contained in gastric gland mucus exhibits anti-H. pylori activity by inhibiting the biosynthesis of CGL, essential for its survival. CGL is biosynthesized by the action of CGL synthase (αCgT) present on the cell wall of H. pylori, in which glucose derived from UDP-glucose binds α1,3 to the hydroxyl group at the 3-position of cholesterol. Cholestenone, on the other hand, is a substance very similar to cholesterol, but with a ketone group at its third position. Therefore, cholestenone cannot be a substrate for CGL synthase, and it is hypothesized that H. pylori cannot biosynthesize CGL in the presence of cholestenone.
Cholestenone is a safe molecule and exhibits antibacterial action by a mechanism of action different from that of conventional antibacterial agents, so it is expected to be a new antibacterial drug against H. pylori including clarithromycin-resistant strain.
###
This work was supported by Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Sciences, Nos. 16K08708 and 18K08419 (M.K.) and19H03441 (J.N.)
Cholestenone functions as an antibiotic against Helicobacter pylori by inhibiting biosynthesis of the cell wall component CGL
Author / Affiliation: Junichi Kobayashi 1,2, *, Masatomo Kawakubo 1, *, Chifumi Fujii 1,3, Nobuhiko Arisaka 1, Masaki Miyashita 1, Yoshiko Sato 1, Hitomi Komura 1, Hisanori Matoba 1, Jun Nakayama 1 (* Co-first author)
1 Department of Molecular Pathology, Shinshu University School of Medicine
2 Department of Internal Medicine, Shinshu University School of Medicine
3 Shinshu University Advanced Area Fusion Research Group Biomedical Research Institute
Proc Natl Adad Sci USA (Proceedings of the American Academy of Sciences)
DOI: 10.1073 / pnas.2016469118
Point of Contact:
3-1-1 Asahi, Matsumoto City, Nagano Prefecture
Jun Nakayama, Professor, Department of Molecular Pathology, Shinshu University School of Medicine
E-mail: [email protected]
Media Contact
Hitomi Thompson
[email protected]
Related Journal Article
http://dx.

{kind=link}