Peer-reviewed / Modelling, Review, and Opinion / People
Credit: The Lancet
Peer-reviewed / Modelling, Review, and Opinion / People
- New World Stroke Organization-Lancet Neurology Commission forecasts future epidemiological and economic impacts of stroke, identifies evidence-based recommendations for improving the four pillars namely: surveillance, prevention, treatment and rehabilitation.
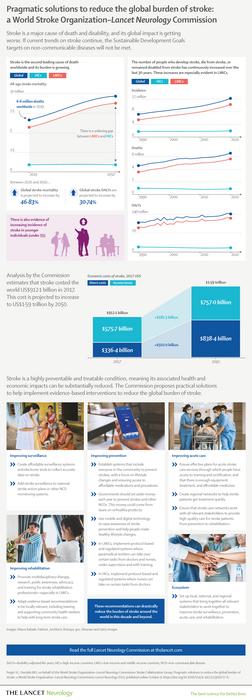
- Epidemiological analysis projects stroke deaths will increase from 6.6 million in 2020 to 9.7 million in 2050, with an ever-widening gap between low- and middle-income countries (LMICs) and high-income countries (HICs). In 2050, 91% of stroke deaths are projected to be in LMICs compared to 9% in HICs, up from 86% in LMICs and 14% HICs in 2020.
- Economic analysis indicates treatment, rehabilitation, and indirect costs of stroke could more than double from US$891 billion in 2020 to up to US$2.3 trillion in 2050.
- Stroke is highly preventable and treatable through the pragmatic solutions recommended by this Commission.
- Implementing and monitoring all of the Commission’s recommendations, which have a firm evidence base, would lead to a drastic reduction in the global burden of stroke thereby curbing its projected burden.
***Infographics available—see notes to editors***
Unless urgent action is taken, the number of people who die from stroke globally is estimated to increase by 50% by 2050 to 9.7 million deaths per year, with annual costs as high as US$2.3 trillion possible, according to a new report on pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization–Lancet Neurology Commission. The authors’ analysis forecasts growing health and economic impacts from stroke between 2020 and 2050, which will disproportionately affect LMICs.
Based on a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the authors make evidence-based pragmatic recommendations to reduce the global burden, including measures to improve stroke surveillance, prevention, acute care, and rehabilitation.
The number of people who suffer a stroke, die from, or remain disabled by the condition globally has almost doubled over the past 30 years, with the vast majority of those affected in LMICs, where prevalence of the condition is increasing at a faster rate than in HICs.
If the current trends continue, one of the World Health Organization’s key Sustainable Development Goals (SDGs) will not be met. SDG 3.4 aims to reduce the 41 million premature deaths from non-communicable diseases – including stroke – by one third by 2030. [1] While achieving these would require US$140 billion in new spending between 2023 and 2030, the financial benefits would outweigh the costs by ten-to-one.
Professor Valery L. Feigin, of Auckland University of Technology, New Zealand, and Commission co-chair, said: “Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars. Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.” [2]
Fast-growing burden of disease, mostly affecting LMICs
In the new Commission, the authors used the Global Burden of Disease (GBD) study methods [3] to provide estimates of stroke burden between 2020 and 2050 in HICs, LMICs and by major GBD world regions and age. Taking into account population growth and aging in most countries, their analysis indicates the number of people who die annually from stroke globally will increase by 50%, rising from 6.6 million in 2020 to 9.7 million in 2050.
The number of stroke deaths in LMICs is projected to rise sharply – widening the gap with HICs – by increasing from 5.7 million in 2020 to 8.8 million in 2050. In contrast, stroke deaths in HICs are estimated to remain largely unchanged at around 900,000 between 2020 and 2050. This indicates that the proportion of global stroke deaths that occur in LMICs will increase from 86% in 2020 to 91% in 2050.
Professor Jeyaraj Pandian, President-Elect of the World Stroke Organization, one of the lead authors of the Commission, and lead author of The Lancet Regional Health – Southeast Asia journal Series on stroke in Southeast Asia [4] said: “Asia accounted for by far the greatest share of global stroke deaths in 2020 (61%, around 4.1 million deaths) and this is forecast to rise to around 69% by 2050 (around 6.6 million deaths). Though smaller relative to Asia, the number of annual global stroke deaths occurring in Sub-Saharan African countries will rise from 6% in 2020 (403,000) to 8% (765,000) in 2050. We have to closely examine what is causing this increase, including the growing burden of uncontrolled risk factors – especially high blood pressure, and lack of stroke prevention and care services in these regions. Without urgent action, stroke deaths in Southeast Asia, East Asia, and Oceania could increase by almost 2 million deaths, from 3.1 million in 2020 to potentially 4.9 million in 2050.” [2]
While the global death rate among people aged over 60 years is predicted to fall by 36% (566 deaths per 100,000 in 2020 to 362 per 100,000 in 2050), among those under 60 years it is predicted to fall by less than 25% (13 per 100,000 in 2020 to 10 per 100,000 in 2050). The Commission authors say the lesser reduction among younger people might relate to increasing levels of diabetes and obesity in this age group.
Huge economic costs, mainly in Asia and Africa
Economic forecasting indicates the combined cost of stroke, including direct costs and loss of income, will rise from US$891 billion per year in 2017 to up to US $2.31 trillion in 2050. The bulk of these economic impacts are forecast to be felt in Asia and Africa.
Projections indicate large increases in direct costs and income losses from stroke in middle-income countries and increases in direct costs in HICs. They also forecast increased economic impacts in low-income countries, but their overall share in global costs is likely to remain small, given their overall low share in global population and stroke cases.
Evidence-based recommendations will greatly reduce the impacts of stroke
To identify key barriers and facilitators to high-quality stroke surveillance, prevention, acute care and rehabilitation, the Commission authors conducted a qualitative analysis of in-depth interviews with 12 stroke experts from six HICs and six LMICs.
Among the major barriers identified were low awareness of stroke and its risk factors (which include high blood pressure, diabetes mellitus, high cholesterol, obesity, unhealthy diet, sedentary lifestyle, and smoking), and limited surveillance data on stroke risk factors, events, management, and outcomes of stroke. Major facilitators included well-developed stroke organisations and networks that can build capacity for stroke care and research, and universal healthcare providing population-wide access to evidence-based stroke care.
Based on the findings of the qualitative analysis, the Commission authors make 12 evidence-based recommendations across stroke surveillance, prevention, acute care, and rehabilitation. Key recommendations include:
- Establishing low-cost surveillance systems to provide accurate epidemiological stroke data to guide prevention and treatment.
- Raising public awareness and action to improve healthy lifestyles and prevent stroke through population-wide use of mobile and digital technologies, such as training and awareness-raising videos and apps.
- Prioritising effective planning of acute stroke care services, capacity building, training, provision of appropriate equipment, treatment and affordable medicines, and adequate resource allocation at national and regional levels.
- Adapting evidence-based recommendations to regional contexts, including training, and support and supervision of community health workers to assist in long-term stroke care.
- Establishing local, national, and regional ecosystems involving all relevant stakeholders to co-create, co-implement and monitor stroke surveillance, prevention, acute care, and rehabilitation.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our Commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans-fats) by each and every government in the world. Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other non-communicable diseases – but also generate a large revenue sufficient to fund not only prevention programmes and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” said Prof. Feigin. [2]
Professor Mayowa O. Owolabi, of the University of Ibadan, Nigeria and Commission co-chair said: “Investing in evidence-based measures to reduce the global burden of stroke will deliver benefits that go far beyond health alone. As well as delivering health and economic benefits relating to stroke, many of our recommendations would also facilitate reductions in poverty and inequality and boost local economies.”
He added, “Every member State of the United Nations has committed to meeting the SDGs but at present few countries are on target to achieve SDG 3.4. Stroke is countable, substantially preventable, treatable, and beatable through the pragmatic solutions recommended by this Commission across the four pillars of the stroke quadrangle (surveillance, prevention, acute care, and rehabilitation). By implementing and monitoring all of the Commission’s recommendations, which have a firm evidence base, the global burden of stroke will be reduced drastically this decade and beyond. Not only will this enable us to meet SDG 3.4, as well as other key SDGs, it will improve brain health and the overall wellbeing of millions of people across the globe now and beyond 2030.” [2,5]
Professor Sheila Martins, of the Universidade Federal of Rio Grande do Sul, Brazil and President of the World Stroke Organization said: “The gaps in stroke services across the world are catastrophic. We need a drastic improvement today, not in 10 years. World Stroke Organization is committed to support and to accelerate the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through the Global Stroke Alliance meetings rotating in the world facilitating the discussions between stroke experts and policy makers, giving the technical support to the governments to elaborate national plans for stroke and to include stroke care in the Universal Health Coverage packages.” [2]
NOTES TO EDITORS
The Commission received funding from the World Stroke Organization, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the National Institutes of Health (USA). It was conducted by researchers from the World Stroke Organization – Lancet Neurology Commission Stroke Collaboration Group. A full list of authors and their institutions is available in the report.
[1] https://www.who.int/data/gho/data/themes/topics/sdg-target-3_4-noncommunicable-diseases-and-mental-health
[2] Quote direct from author and cannot be found in the text of the Article.
[3] Previous estimates of the burden of stroke, done by the Global Burden of Disease study (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31694-5), forecasted health impacts until 2040. However, the Commission authors say effective long-term healthcare planning requires projections for at least the next three decades.
[4] The Lancet Regional Health – Southeast Asia journal Series on stroke in Southeast Asia will be available via www.thelancet.com/series/Stroke-Southeast-Asia at 23:30 UK time on Monday 9 October. For embargoed access to the Series please contact The Lancet press office.
[5] Owolabi MO, Leonardi M, Bassetti C, et al. Global synergistic actions to improve brain health for human development. Nat Rev Neurol 2023; 19: 371–83.
The labels have been added to this press release as part of a project run by the Academy of Medical Sciences seeking to improve the communication of evidence. For more information, please see: http://www.sciencemediacentre.org/wp-content/uploads/2018/01/AMS-press-release-labelling-system-GUIDANCE.pdf if you have any questions or feedback, please contact The Lancet press office [email protected]
IF YOU WISH TO PROVIDE A LINK FOR YOUR READERS, PLEASE USE THE FOLLOWING, WHICH WILL GO LIVE AT THE TIME THE EMBARGO LIFTS: www.thelancet.com/commissions/global-burden-stroke
Journal
The Lancet Neurology
Method of Research
Systematic review
Subject of Research
People
Article Title
Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization–Lancet Neurology Commission
Article Publication Date
9-Oct-2023
COI Statement
VLF states that the free Stroke Riskometer app and PreventS-MD webapp
are owned and copyrighted by AUT Ventures, which is owned by his
employer, Auckland University of Technology (Auckland, New Zealand).
VLF has no financial relationship with the apps, but AUT Ventures
intends to commercialise PreventS-MD via its social enterprise business,
for which VLF serves as chief scientific advisor. PreventS-MD was not
involved in any aspect of the design, conduct, analysis, or content of this
Commission. GAF has received grants from Novartis, consulting fees
from CSL Behring, and honoraria from Astellas and Bayer; has served on
data safety monitoring boards, data-monitoring committees, and steering
committees for Pharmagenesis and Boehringer Ingelheim; and is a nonexecutive director of the UK National Institute for Health and Care
Excellence and a trustee of Health Services Research UK. DCG has
received travel support from the World Federation for Neurorehabilitation
and Conventus Travel, and is a past president of the World Federation for
Neurorehabilitation. WH has participated on data safety monitoring
boards for IFS Institut für anwendungsorientierte Forschung und
klinische Studien and Imperical College, London, and is a past president
of the World Stroke Organization. GJH has received consultation fees
from Janssen Research and Development, Bristol Myers Squibb, and
Bayer, and has participated on data safety monitoring boards for Janssen
Research and Development. PL has received honoraria from Pfizer,
Boehringer Ingelheim, and RAPID-AI iSchemaView; has received travel
support from Angels–Boehringer Ingelheim; has participated on data
safety monitoring boards and steering committees for Pfizer and
Janssen; and is the president of the Chilean Stroke Association and vicepresident of the Iberoamerican Stroke Society. BN has received honoraria
for serving on data safety monitoring boards work for Simbec-Orion. TP
is a member of the Data Safety Monitoring Board for a publicly funded
trial in Germany, with public grant money paid to his institution. AR has
received honoraria from the University of Texas at Austin (Austin, TX,
USA) and Medical College of Virginia (Richmond, VA, USA), and travel
support from Fiji National University. PNS is a leader or member of
advisory boards for Medtronic and the Angels Initiative (funded by
Boehringer-Ingelheim). DY has served as consultant for the Athersys,
Johnson & Johnson, Medtronic, Rapid Medical, Gravity Medical
Technology, Guidepoint Global, Poseydon, Vascular Dynamics, Royal
Caribbean Cruises, and Stryker; holds stocks or stock options in Athersys,
Poseydon, and Rapid Medical; has received honoraria payments from
Emory University (Atlanta, GA, USA); and is founder and global co-chair
of the Society for Vascular and Interventional Neurology’s Mission
Thrombectomy. All other authors declare no competing interests.


{kind=link}