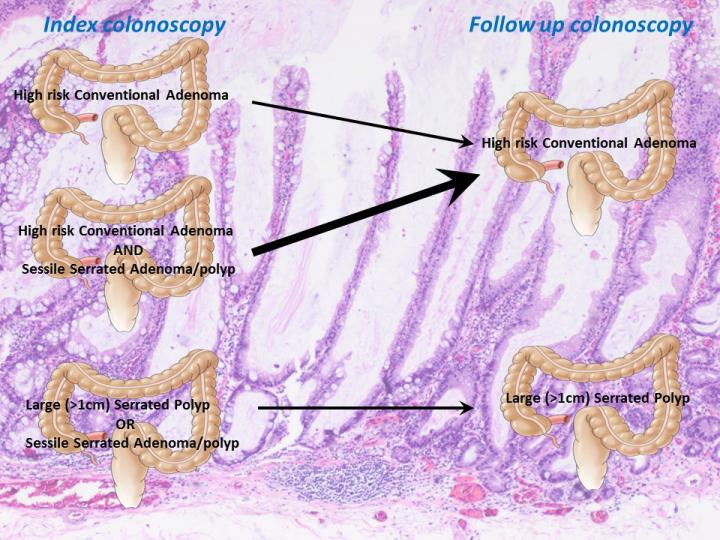
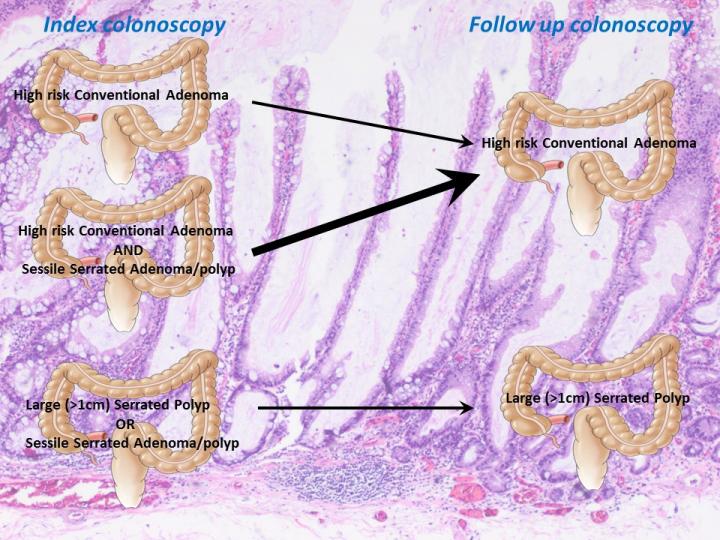
Credit: Joseph Anderson, et al.
LEBANON, NH – Most colorectal cancer develops from precursors known as polyps, the most common and well researched of which are conventional adenomas. Conventional adenomas often progress to colorectal cancer through an intermediate step called high-risk adenomas. Another type of polyp known as serrated polyps, may precede up to 15% of colorectal cancer. Serrated polyps may occur in up to 20% of all adults over 50 years of age, however, when it comes to progression to colorectal cancer, less is known about serrated polyps than conventional adenomas. A Dartmouth research team led by Joseph Anderson, MD, MHCDS, used data from the New Hampshire Colonoscopy Registry (NHCR), led by Lynn Butterly, MD, to examine the risk of developing future high-risk adenomas in people with serrated polyps. They found that when the combination of serrated polyps and high-risk adenomas was present, so was a higher risk of future high-risk adenomas.
The team identified a subgroup of individuals from the NHCR with serrated polyps, hypothesizing that they may be at a higher risk for high-risk adenomas, and thus colorectal cancer, than people with high-risk adenomas alone. "We found that while people with serrated polyps were at increased risk for future serrated polyps, they were not at risk for future high-risk adenomas. Not surprisingly, people with high-risk adenomas were at increased risk for high-risk adenomas," said Anderson. "However, we made a novel observation that people with both serrated polyps and high-risk adenomas had a risk for future high-risk adenomas that was substantially higher than even people with high-risk adenomas alone." The team's findings, "Risk of Metachronous High-risk Adenomas and Large Serrated Polyps in Individuals With Serrated Polyps on Index Colonoscopy: Data from the New Hampshire Colonoscopy Registry," was recently published in Gastroenterology and will be the first paper presented at the American College of Gastroenterology's World Congress of Gastroenterology conference in October, 2017. The data will be presented in the President's Plenary Session, which features the top abstracts at the national meeting.
Several important aspects of the NHCR allowed the team to carry out their study. The first is the size of the registry. The NHCR is a population-based colonoscopy registry that has been collecting and analyzing data on colonoscopies across New Hampshire since 2004 and contains data on over 150,000 colonoscopies.
Next is the thoroughness of NHCR data collection. Consenting participants complete a questionnaire prior to colonoscopy, including demographic characteristics, health history, and known risk factors for colorectal cancer. A procedure form is completed during or immediately following colonoscopy and records the indication for the colonoscopy, findings (location, size and specific treatment of polyps, cancer, or other findings), type and quality of bowel preparation, sedation medication, anatomical landmark reached during the procedure, withdrawal time, follow-up recommendations, and immediate complications. The NHCR requests pathology reports for all colonoscopies with tissue biopsies or excisions directly from each pathology laboratory. Trained NHCR staff then link polyp level pathology data to information from the colonoscopy procedure form in the NHCR database.
The NHCR also provides a longitudinal nature of the data collection. "We follow patients at each successive colonoscopy and can examine the risk that patients can have for future polyps based on an index exam," said Anderson. "The NHCR provided data for a large group of individuals who had both an index and follow up colonoscopy allowing us to address the important clinical question of risk for people with serrated polyps."
The team's data have some important implications. "We have identified a subgroup of individuals with both high-risk adenomas and serrated polyps who may need more intense surveillance such as increased frequency of colonoscopies," said Anderson. "We also observed that having serrated polyps on index exam is associated with an increased risk for future serrated polyps but not high-risk adenomas. Examining rates of serrated polyps rather than high-risk adenomas on follow-up colonoscopy may be the best way to monitor the success of surveillance in people with serrated polyps."
Looking ahead, Anderson's team will dig further into understanding how the risk factors (such as age, sex, smoking, alcohol intake, exercise, education level and family history of colorectal cancer) and molecular mutations found in individuals with both serrated polyps and high-risk adenomas can help identify others who may also be at risk for having both serrated polyps and high-risk adenomas, as these individuals may have a different, higher risk profile for colorectal cancer.
###
Joseph Anderson, MD, MHCDS, is an Associate Professor of Medicine at Dartmouth's Geisel School of Medicine, Gastroenterologist at the Department of Veterans Affairs Medical Center in White River Junction, VT, and co-Investigator at the New Hampshire Colonoscopy Registry, a Dartmouth-Hitchcock Norris Cotton Cancer Center-sponsored initiative.
About Norris Cotton Cancer Center at Dartmouth-Hitchcock
Norris Cotton Cancer Center combines advanced cancer research at Dartmouth's Geisel School of Medicine with patient-centered cancer care provided at Dartmouth-Hitchcock Medical Center in Lebanon, NH, at Dartmouth-Hitchcock regional locations in Manchester, Nashua and Keene, NH, and St. Johnsbury, VT, and at partner hospitals throughout New Hampshire and Vermont. It is one of 49 centers nationwide to earn the National Cancer Institute's "Comprehensive Cancer Center" designation. Learn more about Norris Cotton Cancer Center research, programs, and clinical trials online at cancer.dartmouth.edu.
Media Contact
Jaime Peyton
[email protected]
603-653-3615
http://www.dhmc.org/webpage.cfm?org_id=796
Related Journal Article
http://dx.doi.org/10.1053/j.gastro.2017.09.011

{kind=link}