Credit: ©Science China Press
Lung Cancer is a leading cause of death worldwide, accounting for an estimated 2.09 million new cases in 2018 according to WHO, which is also the leading cause of cancer-related mortality in China [1].
Immunotherapy has been recognized as one of the most significant breakthroughs in lung cancer therapy during the last decade. Immune-oncology (I-O) can be classified into three categories: (1) active immunity includes vaccines, cytokines, and checkpoint inhibitors; (2) passive immunity includes adoptive cell infusion and targeted monoclonal antibodies; (3) hybrid immunity are combined of active and passive methods. Among them, Immune checkpoints were considered as the most promising targets, whose existence helps to dampen or terminate immune activity to guard against autoimmunity and allow for self-tolerance in normal physiological conditions. However, these immune checkpoint pathways can be tricked and hijacked by tumors to evade the attack of immunity system. Checkpoint inhibitors can reactivate the antitumor immunity, delay tumor growth and lengthen the survival by blocking this pathway.
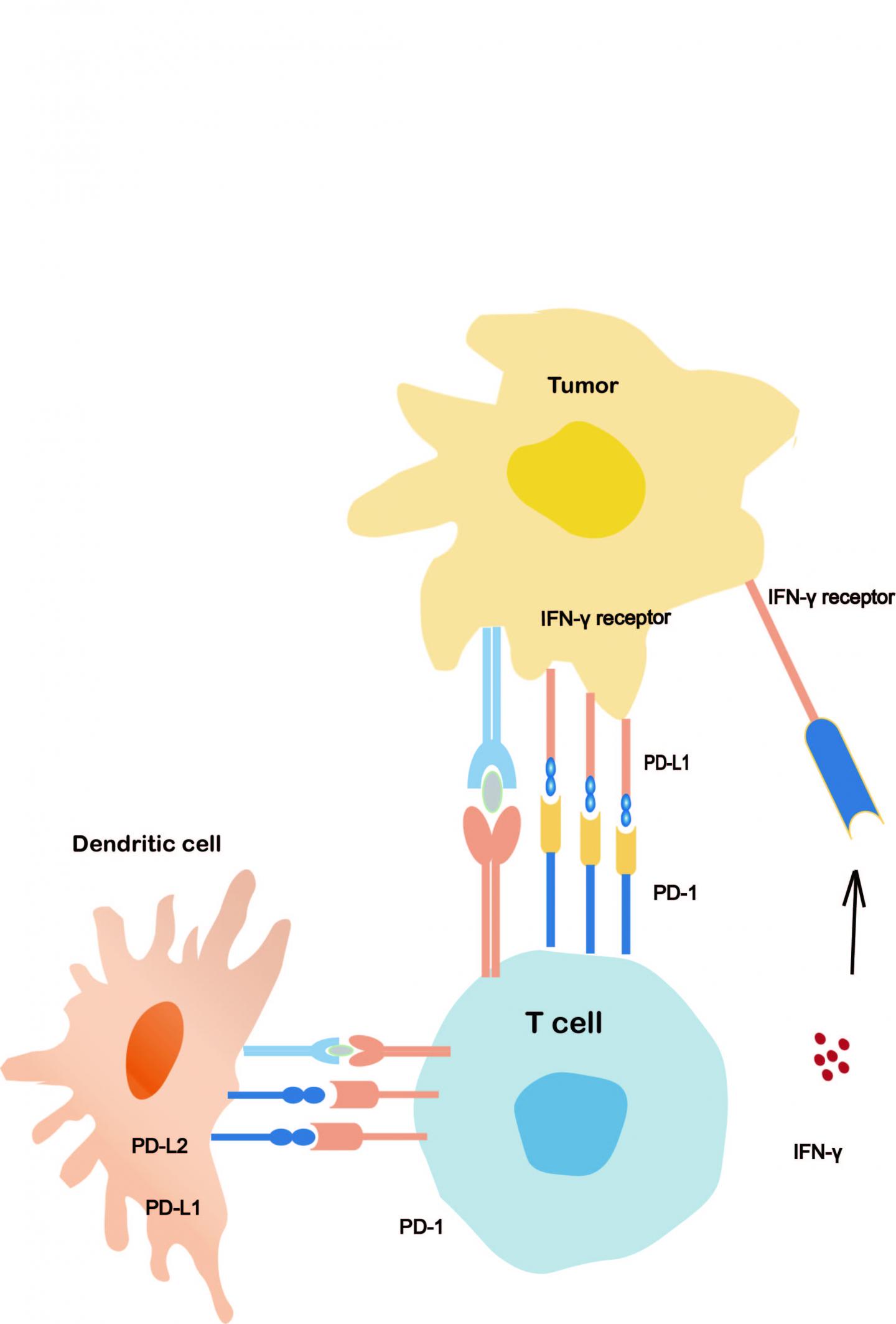
PD-1 is a member of CD28 family which is expressed in several kinds of immune cells, especially in activated CD8+T cells, CD4+T cells, and B cells in peripheral tissues[2].PD-1 has two binding ligands, PD-L1(B7-H1 or CD274) and PDL2(B7-DC or CD273). PD-L1 is expressed on activated T cells, B cells, macrophages, dendritic cells and cancer cells, and the expression of PD-L2 is limited, mainly in activated macrophages, dendritic cells and a small number of tumor cells. The binding of PD-1/PD-L1 suppresses the proliferation, ¬¬survival of the cytotoxic T lymphocyte, induces the apoptosis process of infiltrative T cells and reduces the production of cytokines [3, 4]. PD-L1 is expressed in 27% to 57% of NSCLC patients [5] .The PD-1/PD-L1 pathway plays a vital role in the immune escape of tumor cells [6, 7]. PD-1 or PD-L1 inhibitors block the inhibitory T-cell signaling, and reactivating the antitumor activity of CD8+ T cells [8]. Tumor cells escape the immune response through the upregulation of PD-L1 to inhibit the action of T cells. Basing on this background, many drugs targeting the PD-1 pathway are under development, and clinical trials of drugs for the PD-1 pathway have been conducted.
However, the proportion of patients who can benefit from ICIs is relatively small. For instance, only 20-25% of NSCLC patients showed a sustainable response to ICIs[9]. Therefore, the discovery and exploration of clinical or biological biomarkers for ICIs is urgent and meaningful. The aim of this approach is to find out the people who may benefit from checkpoint inhibitors and improve the whole cost-effectiveness. However, on account of the complexity of the relationship between tumor and immune-microenvironment, the factors affect the clinical effect of ICIs are multi-dimensional, such as PD1/PD-L1 expression, tumor mutation burden (TMB), Specific Gene Mutations and even Gut Microbiome, et al.
In this brightness and challenges, researchers describe the progress made so far, including the PD-1/PD-L1 inhibitors in clinical practice in lung cancer, followed by their understanding of how biomarkers can be utilized to figure out the most likely beneficiary from ICIs. In conclusion, this article highlights the current clinical trials for the accumulation of knowledge of primary and acquired resistance to improve the clinical outcomes.
###
This research was funded by the National Key R&D Program of China (2016YFC1303300), the National Natural Science Foundation of China (81672272), Shanghai Municipal Science & Technology Commission Research Project (17431906103), Shanghai Chest Hospital Project of Collaborative Innovation?YJXT20190105?and the Clinical Research Plan of SHDC (16CR3005A).
[1] W. Chen, R. Zheng, H. Zeng, S. Zhang, Epidemiology of lung cancer in China, Thoracic cancer, 6 (2015) 209-215.
[2] Y. Agata, A. Kawasaki, H. Nishimura, Y. Ishida, T. Tsubata, H. Yagita, T. Honjo, Expression of the PD-1 antigen on the surface of stimulated mouse T and B lymphocytes, Int Immunol, 8 (1996) 765-772.
[3] K. Karwacz, C. Bricogne, D. MacDonald, F. Arce, C.L. Bennett, M. Collins, D. Escors, PD-L1 co-stimulation contributes to ligand-induced T cell receptor down-modulation on CD8+ T cells, EMBO Mol Med, 3 (2011) 581-592.
[4] D.M. Pardoll, The blockade of immune checkpoints in cancer immunotherapy, Nat Rev Cancer, 12 (2012) 252-264.
[5] Y.B. Chen, C.Y. Mu, J.A. Huang, Clinical significance of programmed death-1 ligand-1 expression in patients with non-small cell lung cancer: a 5-year-follow-up study, Tumori, 98 (2012) 751-755.
[6] Y. Iwai, M. Ishida, Y. Tanaka, T. Okazaki, T. Honjo, N. Minato, Involvement of PD-L1 on tumor cells in the escape from host immune system and tumor immunotherapy by PD-L1 blockade, Proc Natl Acad Sci U S A, 99 (2002) 12293-12297.
[7] J.M. Taube, R.A. Anders, G.D. Young, H. Xu, R. Sharma, T.L. McMiller, S. Chen, A.P. Klein, D.M. Pardoll, S.L. Topalian, L. Chen, Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape, Sci Transl Med, 4 (2012) 127ra137.
[8] E.B. Garon, N.A. Rizvi, R. Hui, N. Leighl, A.S. Balmanoukian, J.P. Eder, A. Patnaik, C. Aggarwal, M. Gubens, L. Horn, E. Carcereny, M.J. Ahn, E. Felip, J.S. Lee, M.D. Hellmann, O. Hamid, J.W. Goldman, J.C. Soria, M. Dolled-Filhart, R.Z. Rutledge, J. Zhang, J.K. Lunceford, R. Rangwala, G.M. Lubiniecki, C. Roach, K. Emancipator, L. Gandhi, K.-. Investigators, Pembrolizumab for the treatment of non-small-cell lung cancer, N Engl J Med, 372 (2015) 2018-2028.
[9] C. Kaderbhaï, Z. Tharin, F. Ghiringhelli, The Role of Molecular Profiling to Predict the Response to Immune Checkpoint Inhibitors in Lung Cancer, Cancers, 11 (2019).
Media Contact
Shun Lu
[email protected]
Related Journal Article
http://dx.



{kind=link}