A surprising mechanism that makes some cancers treatment-resistant has been discovered by Weill Cornell Medicine and NewYork-Presbyterian investigators. The mechanism, which involves the shuttling of messenger RNAs (mRNAs) from the nucleus to the cytoplasm, ultimately facilitates DNA repair in cancer cells. These cancer cells can thereby thwart treatments aimed at damaging their DNA.
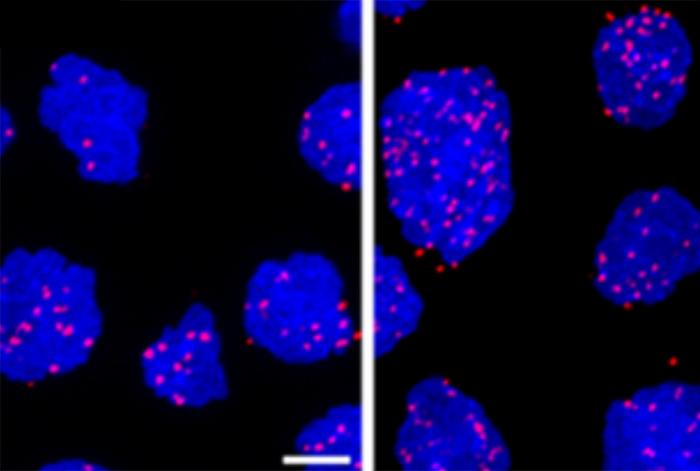
Credit: Weill Cornell Medicine
A surprising mechanism that makes some cancers treatment-resistant has been discovered by Weill Cornell Medicine and NewYork-Presbyterian investigators. The mechanism, which involves the shuttling of messenger RNAs (mRNAs) from the nucleus to the cytoplasm, ultimately facilitates DNA repair in cancer cells. These cancer cells can thereby thwart treatments aimed at damaging their DNA.
In a project encompassing both fundamental research and clinical studies they demonstrated that a combination of approved chemotherapies, one of which targets the DNA repair-facilitating mechanism, could help treat these persistent cases. While the work, published Oct. 6 in Cancer Research, focused on diffuse large B-cell lymphoma (DLBCL), the findings likely apply to other cancer types as well.
DLBCL is the most common form of lymphoma, affecting about 30,000 patients annually in the United States alone. First-line therapies cure about two thirds of patients, “but for people who aren’t cured or who relapse, they historically had poor outcomes with standard chemotherapy-based treatment approaches,” said co-lead author Dr. Sarah Rutherford, an assistant professor of medicine at Weill Cornell Medicine and a hematologist/oncologist at NewYork-Presbyterian/Weill Cornell Medical Center. The other co-lead author is Dr. Rossella Marullo, an instructor in medicine at Weill Cornell Medicine.
Previous research had demonstrated that treatment-resistant DLBCL cells often express high levels of a protein called XPO1. In 2019, the U.S. Food and Drug Administration approved a new drug, selinexor, that was designed to target XPO1 and inhibit its activity. The drug, which hinders the growth of lymphoma cells expressing high levels of the protein, is used to treat these refractory cases. Selinexor has helped many, but not all patients with treatment-resistant disease.
“Selinexor is effective by itself, it’s just not as effective as we’d like it to be,” said Dr. Rutherford, who is also a member of the Sandra and Edward Meyer Cancer Center at Weill Cornell Medicine. That’s driven her to search for ways to improve the drug’s efficacy.
Meanwhile, Dr. Rutherford’s colleagues were trying to learn more about exactly how selinexor works. Its target, XPO1, transports hundreds of proteins, and certain RNAs, out of the cell nucleus, primarily to separate the pool of proteins that should not be present in the nucleus, such as ribosomal proteins.
However, the investigators found that some of these XPO1-exported proteins are also bound to mRNA molecules; thus, these mRNAs are exported out of the cell nucleus into the cytoplasm where they can be translated into proteins. This new mechanism indicates that the quantity and activity of XPO1 in a cell can therefore affect the expression levels of numerous genes.
“We found that it’s not just regulating a few proteins, it’s coordinating these big programs, allowing cells to rapidly adjust their proteome and survive different kinds of stress that cancer cells encounter all the time,” said senior author Dr. Leandro Cerchietti, the Richard Stratton Associate Professor of Hematology and Oncology and a member of the Meyer Cancer Center at Weill Cornell Medicine.
Taking some treatment resistant DLBCL cells from patients and grafting them into preclinical models, the researchers found that higher levels of XPO1 ultimately increases the expression of genes that protect cells against death from DNA damage. Inhibiting XPO1 in those models with selinexor increased the lymphomas’ sensitivity to DNA-damaging chemotherapies and immune-based treatments.
“We were excited, and based on some of Dr. Cerchietti’s research, we thought selinexor would likely synergize with other chemotherapies,” said Dr. Rutherford. To test that in patients, she initiated a phase 1 clinical trial, aiming to determine whether such a combination would be safe, and if so at what doses. The trial, which primarily enrolled patients with treatment-resistant DLBCL, showed that the combined regimen is not only safe, but appears to work. Though the data set is too small to draw definitive conclusions, several patients had better outcomes than expected.
Dr. Rutherford is eager to continue testing and refining the new regimens in follow-up trials. “It has been a really exceptional time over the last four years or so in this disease, where we now have many more therapies than we did when we first started the trial,” she said.
Because every cell in the body expresses XPO1, the new results are likely to have broader applications. “There are other tumors in which XPO1 is overexpressed, so it’s really a nice backbone to build on,” said Dr. Cerchietti.
Many Weill Cornell Medicine physicians and scientists maintain relationships and collaborate with external organizations to foster scientific innovation and provide expert guidance. The institution makes these disclosures public to ensure transparency. For this information, see profile for Dr. Sarah Rutherford.
Journal
Cancer Research


{kind=link}