The American College of Cardiology (ACC) and the American Heart Association (AHA), along with several other leading medical associations, have issued a new guideline for preventing and optimally managing atrial fibrillation (AFib). The guideline was jointly published today in the Journal of the American College of Cardiology and Circulation.
Credit: Journal of the American College of Cardiology
The American College of Cardiology (ACC) and the American Heart Association (AHA), along with several other leading medical associations, have issued a new guideline for preventing and optimally managing atrial fibrillation (AFib). The guideline was jointly published today in the Journal of the American College of Cardiology and Circulation.
Atrial fibrillation, or AFib, is the most common type of heart rhythm disorder (arrhythmia), affecting over 6 million Americans, and the number is expected to double by 2030. AFib causes a variety of symptoms, including fast or chaotic heartbeat, fatigue, shortness of breath, and chest pain, and causes about 450,000 hospitalizations each year, according to the Centers for Disease Control and Prevention. If untreated, AFib can lead to or exacerbate heart failure, and it significantly increases a person’s risk of stroke.
The updated guideline calls for a stronger, more prescriptive focus on healthy lifestyle habits to prevent or lessen the burden of AFib, as well as early and more aggressive rhythm control in general, including upgraded recommendations for catheter ablation as first line therapy to prevent disease progression. Also detailed is updated guidance on the management of heart rate and rhythm medications, use of anticoagulants, and when to temporarily pause or stop these therapies.
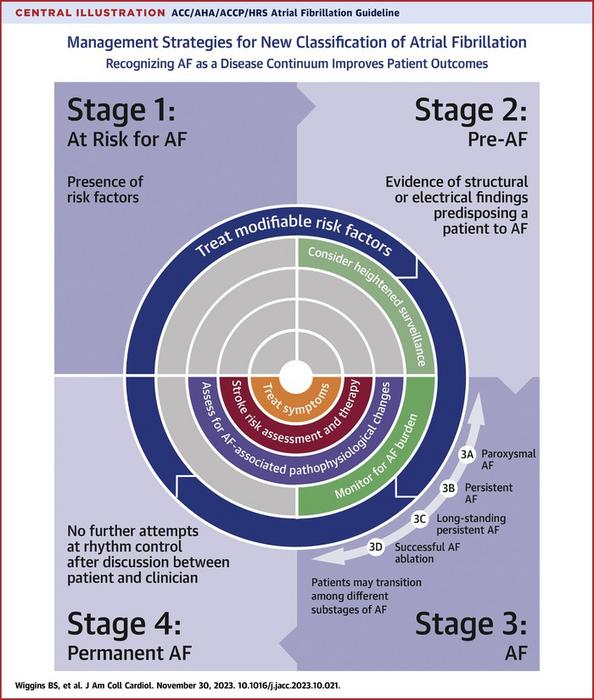
Further, the guideline sets forth a new way to classify AFib, using stages, that reinforces the continuum of the disease and underscores the need to use a variety of strategies at the different stages, including prevention, lifestyle and risk factor modification, screening, and therapy. Previously, AFib was primarily classified based only on arrhythmia duration, which, although useful, tended to emphasize specific therapeutic interventions as opposed to a more holistic and multidisciplinary management approach.
“This is a complex disease. It’s not just an isolated disorder of the heart’s rhythm, and we now know that the longer someone is in AFib, the harder it is to get them back to normal sinus rhythm,” said Jose Joglar, MD, professor of cardiac electrophysiology at UT Southwestern Medical Center in Dallas and chair of the writing committee. “The new guideline reinforces the urgent need to approach AFib as a complex cardiovascular condition that requires disease prevention, risk factor modification, as well as optimizing therapies and patients’ access to care and ongoing, long-term management.”
There is clearer focus on risk factor modification—for example, weight loss and obesity prevention, physical activity, smoking cessation, limiting alcohol, and controlling blood pressure and other comorbidities—to help prevent AFib or ameliorate any recurrences or worsening of the disease. Recommendations are intentionally prescriptive in nature so that clinicians can give patients specific goals and provide a clearer road map for how they can take steps to live healthier and change the course of their disease.
“Many patients don’t know where to start when they are given advice about lifestyle modification, so we are very specific with our recommendations,” Joglar said. “For example, instead of saying ‘you need to exercise,’ which is largely unhelpful to patients, we recommend talking with patients about what types of physical activity works for them and how many minutes they should be active each day or each week.”
The good news for many people, he added, is that your morning coffee is okay when it comes to AFib, according to the latest data, but if individuals notice that caffeine makes them feel bad, they should skip it.
Catheter ablation was given the highest Class 1 treatment recommendation for appropriately selected patients, including those with heart failure with reduced ejection fraction. Catheter ablation is a minimally invasive procedure that disables portions of heart tissue that cause irregular heart rhythms.
“In the past, catheter ablation was considered a second line option after medications were tried and failed, and now we are advising that, in select AFib patients, you can proceed to catheter ablation as a first option,” Joglar said, adding that recent data showed catheter ablation to be more effective than medications in preventing disease progression in some populations.
Still, he emphasized the need for a multipronged approach for better success. Because AFib and heart failure frequently overlap, there is a section specific to key considerations for these patients, reinforcing aggressive rhythm control to help heart function to recover.
Although the guideline continues to endorse use of the CHA2DS2-VASc score as the predictor of choice to determine patients’ stroke risk, other risk calculators should be considered when uncertainty exists or when other risk factors need to be included. For example, kidney disease is not included in CHA2DS2-VASc. Patients, especially those at intermediate risk, may benefit from evaluation with more than one risk calculator because some work better than others in different patient populations, or other factors need to be considered. For example, recommendations for blood thinners should be based on a comprehensive yearly thromboembolic event risk rather than on a specific score.
“The new guideline gives clinicians flexibility to use other predictive tools, and we hope this will also enhance communication and shared decision-making with patients,” Joglar said, adding that there is enhanced focus on the use of left atrial appendage closure devices for stroke prevention. This device sits in the heart’s left atrial appendage, where blood clots often form, to prevent them from getting into the bloodstream.
Similar to other chronic conditions, such as high blood pressure or Type 2 diabetes, Joglar said we “now have a better understanding and more tools to prevent, treat and also mitigate the risk of AFib so that we can improve patient outcomes.”
The writing committee was comprised of cardiologists, cardiac electrophysiologists, surgeons, pharmacists, and patient representatives/lay stakeholders.
Additional Resources:
- After Nov. 30, view the manuscript online in JACC or Circulation.
- ACC.org Guideline Hub (Hub update available at embargo lift)
- JACC.org Guideline Hub (Hub available at embargo lift)
- CardioSmart.org (Hub update available at embargo lift)
- AHA health information: About Atrial Fibrillation
- AHA AFib resources for patients and professionals
- AHA patient support network: My AFib Experience
The American College of Cardiology (ACC) is the global leader in transforming cardiovascular care and improving heart health for all. As the preeminent source of professional medical education for the entire cardiovascular care team since 1949, ACC credentials cardiovascular professionals in over 140 countries who meet stringent qualifications and leads in the formation of health policy, standards and guidelines. Through its world-renowned family of JACC Journals, NCDR registries, ACC Accreditation Services, global network of Member Sections, CardioSmart patient resources and more, the College is committed to ensuring a world where science, knowledge and innovation optimize patient care and outcomes. Learn more at www.ACC.org or follow @ACCinTouch.
The American Heart Association is a relentless force for a world of longer, healthier lives. We are dedicated to ensuring equitable health in all communities. Through collaboration with numerous organizations, and powered by millions of volunteers, we fund innovative research, advocate for the public’s health and share lifesaving resources. The Dallas-based organization has been a leading source of health information for nearly a century. Connect with us on heart.org, Facebook, X or by calling 1-800-AHA-USA1.
###
Journal
Journal of the American College of Cardiology


{kind=link}