Findings from a nationwide, multicenter study led by Johns Hopkins Medicine and the Johns Hopkins Bloomberg School of Public Health suggest that patients with COVID-19 have less chance of developing post-COVID conditions — commonly known as long COVID — if they receive early treatment with plasma from convalescent (recovered) COVID patients that contain antibodies against SARS-CoV-2, the virus that causes COVID-19.
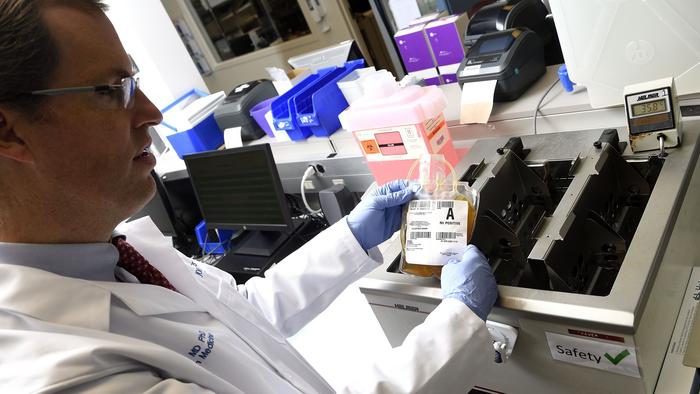
Credit: Will Kirk, Johns Hopkins University
Findings from a nationwide, multicenter study led by Johns Hopkins Medicine and the Johns Hopkins Bloomberg School of Public Health suggest that patients with COVID-19 have less chance of developing post-COVID conditions — commonly known as long COVID — if they receive early treatment with plasma from convalescent (recovered) COVID patients that contain antibodies against SARS-CoV-2, the virus that causes COVID-19.
The new research, first posted online today in mBio, a journal from the American Society for Microbiology, is a follow-up investigation to the 2021 clinical trial that showed convalescent plasma is an effective and safe option as an early outpatient treatment for COVID-19. The latest study looked at the long-term outcomes of a large portion of the participants from the 2021 clinical trial.
“Following our initial study, health care professionals kept SARS-CoV-2 antibody-rich blood plasma available in their blood banks as part of the treatment arsenal against COVID-19 in people who are immunocompromised; and now, our new findings show it also may lower the risk of post-COVID conditions,” says study co-lead author David Sullivan, M.D., professor of molecular microbiology and immunology at the Johns Hopkins Bloomberg School of Public Health with a joint appointment in infectious diseases at the Johns Hopkins University School of Medicine.
The original outpatient early treatment clinical trial was conducted between June 2020 and October 2021. The researchers provided 1,181 randomized participants with one unit each of either polyclonal high-titer convalescent plasma (containing a concentrated mixture of antibodies specific to SARS-CoV-2) or placebo control plasma (with no SARS-CoV-2 antibodies). The participants were 18 and older, and had tested positive for SARS-CoV-2 within eight days prior to transfusion. A successful outcome was defined as not requiring hospitalization within 28 days after plasma transfusion.
The original clinical trial found that 17 participants out of 592 (2.9%) who received the convalescent plasma required hospitalization within 28 days of their transfusion, while 37 out of 589 (6.3%) who received placebo control plasma did. This translated to a relative risk reduction for hospitalization of 54%.
As part of the clinical trial, 882 participants also were evaluated for their levels of 21 different cytokines and chemokines at screening, and at 14 days and 90 days after they received either convalescent plasma or placebo control plasma. Cytokines and chemokines are signaling proteins secreted by cells in response to infection, and as a result, activate specific immune system functions such as inflammation. In turn, excessive or unchecked inflammation is believed to be a key factor in the development of post-COVID conditions.
For the latest study, the researchers used the cytokine and chemokine measurements, along with reports by patients of any post-COVID conditions at the 90-day examination, to determine if there was any association between early convalescent plasma therapy and long COVID symptoms. Statistical analyses were conducted to validate the findings, after adjusting for other factors that could make someone more prone to post-COVID conditions, such as demographics (e.g., age and race), competing diseases (e.g., diabetes) and vaccine status.
At 90 days after receiving either convalescent or control plasma, 590 (66.9%) of the study participants showed no post-COVID conditions, while 292 (33.1%) did. Of the latter group, the most commonly reported symptoms were fatigue and anosmia (loss of smell).
Levels of cytokines and chemokines were elevated at screening for most of the study participants, and decreased more by day 90 in those who had received convalescent plasma,” says study senior author Aaron Tobian, M.D., Ph.D., director of the Transfusion Medicine Division and professor of pathology at the Johns Hopkins University School of Medicine.
Additionally, study participants who had higher-than-normal levels of one particular cytokine, interleukin-6 (IL6), at screening were more likely to be among those with post-COVID symptoms by day 90. IL6 is known to trigger an inflammatory response in humans.
“Our study is among the first to show that elevation of IL6 early after the onset of infection is associated with post-COVID conditions,” says study co-lead author Kelly Gebo, M.D., M.P.H., professor of medicine at the Johns Hopkins University School of Medicine. “While cytokine levels decreased throughout the study population from infection to day 90, they dropped more significantly in those who received convalescent plasma early in the course of their illness. So, it appears that when IL6 levels remain elevated during the COVID-19 recovery phase, it likely contributes to post-COVID conditions.”
Future studies, says Gebo, could examine the impact of anti-IL6 agents combined with other treatments against COVID-19 among outpatients.
Because of the large number of co-authors on this study, their names, financial disclosures and conflict-of-interest statements are not listed here. That information may be found in the published paper.
The study was principally funded by the U.S. Department of Defense’s Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense (DOD JPEO-CBRND), in collaboration with the Defense Health Agency (DHA). Initial support was received from the Bloomberg Philanthropies and the state of Maryland, with additional support coming from National Institute of Allergy and Infectious Diseases grant 3R01AI152078-01S1 and the agency’s Division of Intramural Research, National Center for Advancing Translational Sciences grant U24TR001609, the Mental Wellness Foundation, the Moriah Fund, Octapharma Plasma, the HealthNetwork Foundation and the Shear Family Foundation.
The views expressed are those of the authors and should not be construed to represent the positions of the U.S. Army or the U.S. Department of Defense. The data and opinions presented do not reflect the view of the U.S. government.
Journal
mBio

{kind=link}